
René Magritte The human condition 1935


Yeadon
Dr. Michael Yeadon says governments are lying to us about Covid-19
"I've spent 40 years training & practice in life science. I have no incentive whatsoever to make this stuff up. What I'm telling you is true — that you're being misled."
Full video: https://t.co/vuFGlOqz4y pic.twitter.com/Qh8vYgllSZ
— Taylor Hudak (@_taylorhudak) August 6, 2021
They’re planning the approval in early September. That will be the last of the FDA’s credibility.
“This is a dystopian world we’re living in,” he said. The public is awash in lies and misinformation about COVID-19 and the vaccines, “they are being misled.”
“Americans, he hopes, will say, “I’m not going to take any of this. I’m seeing everybody around me get sick and dying. Let me just go ahead and get vaccinated.'”
• Fauci: ‘Flood’ Of Covid-19 Vaccine Mandates After Full FDA Approval (USAT)
As soon as the Food and Drug Administration issues a full approval for a COVID-19 vaccine, there will be “a flood” of vaccine mandates at businesses and schools across the nation, Dr. Anthony Fauci told USA TODAY’s editorial board on Friday. Mandates aren’t going to happen at the federal level, but vaccine approval will embolden many groups, he predicted. “Organizations, enterprises, universities, colleges that have been reluctant to mandate at the local level will feel much more confident,” he said. “They can say, ‘If you want to come to this college or this university, you’ve got to get vaccinated. If you want to work in this plant, you have to get vaccinated. If you want to work in this enterprise, you’ve got to get vaccinated. If you want to work in this hospital, you’ve got to get vaccinated.'”
Fauci doesn’t see more lockdowns in the nation’s future. They were issued early in the pandemic to keep hospitals from being overwhelmed, known as “flattening the curve.” “The rationale for shutting down was that the hospital system would not be able to handle the surge of cases because everybody was getting sick,” he said. With upwards of 70% of adults having had at least one dose of vaccine, the epidemic has shifted to one of the unvaccinated, he said. “When you walk into a hospital, what you’re going to see is a lot of young people, some of whom are seriously ill, but you’re not seeing an overwhelming outstripping of the capability of the hospitals throughout the country,” he said. While he’s attacked online and in conservative media every day, Fauci said he worries less about himself than for the nation as a whole.
“This is a dystopian world we’re living in,” he said. The public is awash in lies and misinformation about COVID-19 and the vaccines, “they are being misled.” With COVID-19 cases rising among the unvaccinated as the highly contagious delta variant spreads, Fauci hopes people’s “better angels” will prevail over the sea of lies on social media. Americans, he hopes, will say, “I’m not going to take any of this. I’m seeing everybody around me get sick and dying. Let me just go ahead and get vaccinated.'”
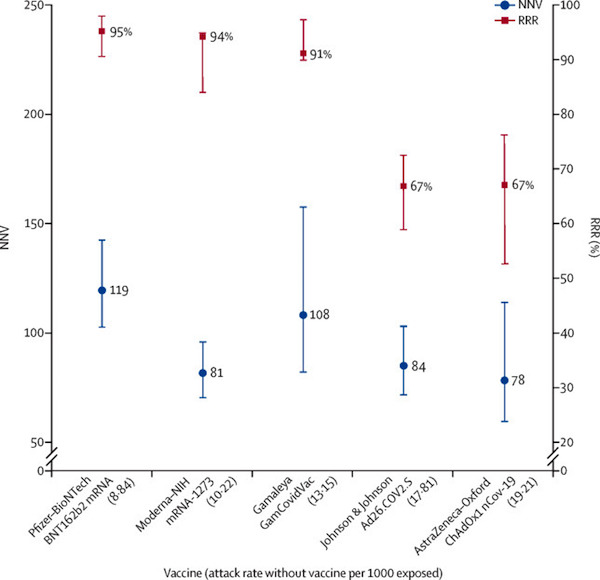
Absolute Risk Reduction = 1·3% for the AstraZeneca–Oxford, 1·2% for the Moderna–NIH, 1·2% for the J&J, 0·93% for the Gamaleya, and 0·84% for the Pfizer–BioNTech vaccines.
• Covid19 Vaccine Efficacy & Effectiveness – The Elephant (Not) In The Room (L.)
Vaccine efficacy is generally reported as a relative risk reduction (RRR). It uses the relative risk (RR)—ie, the ratio of attack rates with and without a vaccine—which is expressed as 1–RR. Ranking by reported efficacy gives relative risk reductions of 95% for the Pfizer–BioNTech, 94% for the Moderna–NIH, 91% for the Gamaleya, 67% for the J&J, and 67% for the AstraZeneca–Oxford vaccines. However, RRR should be seen against the background risk of being infected and becoming ill with COVID-19, which varies between populations and over time. Although the RRR considers only participants who could benefit from the vaccine, the absolute risk reduction (ARR), which is the difference between attack rates with and without a vaccine, considers the whole population. ARRs tend to be ignored because they give a much less impressive effect size than RRRs: 1·3% for the AstraZeneca–Oxford, 1·2% for the Moderna–NIH, 1·2% for the J&J, 0·93% for the Gamaleya, and 0·84% for the Pfizer–BioNTech vaccines.
ARR is also used to derive an estimate of vaccine effectiveness, which is the number needed to vaccinate (NNV) to prevent one more case of COVID-19 as 1/ARR. NNVs bring a different perspective: 81 for the Moderna–NIH, 78 for the AstraZeneca–Oxford, 108 for the Gamaleya, 84 for the J&J, and 119 for the Pfizer–BioNTech vaccines. The explanation lies in the combination of vaccine efficacy and different background risks of COVID-19 across studies: 0·9% for the Pfizer–BioNTech, 1% for the Gamaleya, 1·4% for the Moderna–NIH, 1·8% for the J&J, and 1·9% for the AstraZeneca–Oxford vaccines. ARR (and NNV) are sensitive to background risk—the higher the risk, the higher the effectiveness—as exemplified by the analyses of the J&J’s vaccine on centrally confirmed cases compared with all cases:8 both the numerator and denominator change, RRR does not change (66–67%), but the one-third increase in attack rates in the unvaccinated group (from 1·8% to 2·4%) translates in a one-fourth decrease in NNV (from 84 to 64).
There are many lessons to learn from the way studies are conducted and results are presented. With the use of only RRRs, and omitting ARRs, reporting bias is introduced, which affects the interpretation of vaccine efficacy.10 When communicating about vaccine efficacy, especially for public health decisions such as choosing the type of vaccines to purchase and deploy, having a full picture of what the data actually show is important, and ensuring comparisons are based on the combined evidence that puts vaccine trial results in context and not just looking at one summary measure, is also important. Such decisions should be properly informed by detailed understanding of study results, requiring access to full datasets and independent scrutiny and analyses.
Doctors 4 Covid Ethics: “Are we about to witness the birth of an entirely new world of autoimmune disease?”
• Leaky Blood Vessels: An Unknown Danger of COVID-19 Vaccination (D4CE)
Dear colleague: Six months ago, we laid out the reasons for our fears that gene-based vaccines were potentially dangerous [1]. These concerns were based primarily on the expectation that the vaccine would through lymphatic transport soon enter the circulation, where it would be taken up by the endothelial cells. These cells would then start producing the spike protein, which would cause them to be attacked and destroyed by cytotoxic Tlymphocytes. The resulting lesions would give rise to platelet activation and blood clot formation. Since then, clotting abnormalities have indeed taken center stage as propagators of adverse events following vaccinations.
Rapid entry of the vaccine into the bloodstream has been confirmed, as has rapid appearance of expressed spike protein in the bloodstream. Activation of clotting is very common even in those without characteristic or lasting symptoms, but the number of grave adverse events caused by this mechanism—heart attack, stroke, cerebral sinus venous thrombosis, and others—is very high. With this letter, your attention is directed to a second autoimmune pathway that will be triggered simultaneously with the activation of cytotoxic T-lymphocytes. We predict that this pathway will cause damage to and leakiness of blood vessels, with consequences that are far-reaching and profound, particularly upon repeated vaccination. This second autoimmune pathway will render booster shots uniquely dangerous.
1. The proposed mechanism
The first injection will induce the expression of spike protein, and the formation of specific antibodies to it. Re-vaccination will lead to a second round of spike protein production, including in endothelial cells. The antibodies, now already present, will bind to these spikes and will direct attack of the complement system to these cells. Neutrophil granulocytes, too, will be activated by antibodies bound to the endothelial cells. Vascular damage and leakage will ensue.1.1. Evidence that SARS-CoV-2 spikes provoke complement attack on vessels
Investigations published last year by Jeffrey Laurence and colleagues [2] have establishedthat spike proteins direct complement attack to the inner vessel lining. The authors showed that spike proteins released from the lungs of COVID-19 patients travelled via the circulation to attach at distant sites to the inner vessel lining, i.e. the endothelial cells. Leukocytes and the complement system became activated precisely at those sites, which resulted in damage and leakiness of the vessels. Why this occurred became evident only recently, through several discoveries that we have discussed in a previous letter to physicians [3]. Specifically, the immune system of all individuals is already primed to respond to coronaviruses including SARS-CoV-2, most likely through cross-immunity with widespread respiratory human coronavirus strains. This immunological memory causes antibody production to commence early on during SARS-CoV-2 infection [4–7]. Thus, antibodies will already be there to bind the spike proteins when these become stranded in the vessel linings. This inevitably triggers activation of the complement cascade.1.2. The effect of booster shots
Repeat injections of gene-based “vaccines” are bound to intensify and reproduce this basic event wherever the newly expressed spike protein appears on the vessel lining. Spike protein-induced complement attack on vessels has been shown to evoke a plethora of skin lesions in COVID-19 patients [8]. These show a striking resemblance to some of those which are now being reported in vaccinated individuals [9]. Complementmediated vascular injury occurring at multiple sites throughout the body will have potentially devastating effects not only on the health of the vaccinated individual, but also on pregnancy and fertility. Complement will also likely potentiate coagulation abnormalities via yet another pathway. Spike protein molecules, known to be released into the bloodstream shortly after vaccination [5] will bind to platelets, marking them as targets for antibody binding. Subsequent attack by complement must be expected to cause platelet destruction, possibly culminating in immune thrombocytopenic purpura. This, too, has been clinically observed after vaccination [10–13]. With regard to long term effects of re-vaccination, what will happen when the “vaccines” seep out of damaged blood vessels and reach the organs of the body? Will gene uptake and spike production then mark each and every cell type for destruction by killer lymphocytes? Are we about to witness the birth of an entirely new world of autoimmune disease?1.3. Conclusion
It is beyond question that repeated vaccinations carry serious and unprecedented risks as outlined above. While government officials, authorities and vaccine manufacturers may remain ignorant of the medical implications of such findings, any physician in possession of this knowledge cannot administer repeated COVID-19 vaccination in good conscience, nor in good faith. Under no circumstances is it acceptable for a doctor to knowingly inflict harm on a patient. ALL PHYSICIANS ARE HEREWITH CALLED ON TO RECONSIDER THE ETHICAL ISSUES SURROUNDING COVID-19 VACCINATION.
Not THAT early…
• Early Signs Covid-19 Vaccines May Not Stop Delta Transmission (R.)
There are early signs that people who have been vaccinated against COVID-19 may be able to transmit the Delta variant of the virus as easily as those who have not, scientists at Public Health England (PHE) said on Friday. The findings chime with those from the U.S. Centers for Disease Control and Prevention, which last week raised concerns that vaccinated people infected with Delta could, unlike with other variants, readily transmit it. read more The highly infectious Delta variant has become the dominant coronavirus type globally, sustaining a pandemic that has already killed more than 4.4 million people, including over 130,000 in Britain. Vaccines have been shown to provide good protection against severe disease and death from Delta, especially with two doses, but there is less data on whether vaccinated people can still transmit it to others.
“Some initial findings … indicate that levels of virus in those who become infected with Delta having already been vaccinated may be similar to levels found in unvaccinated people,” PHE said in a statement. “This may have implications for people’s infectiousness, whether they have been vaccinated or not. However, this is early exploratory analysis and further targeted studies are needed to confirm whether this is the case.” PHE said that of confirmed Delta cases that had ended up hospitalised since July 19, 55.1% were unvaccinated, while 34.9% had received two doses of a COVID-19 vaccine. Nearly 75% of the British population has had two vaccine doses, and PHE said that “as more of the population gets vaccinated, we will see a higher relative percentage of vaccinated people in hospital”.
Separately, PHE said another variant, known as B.1.621, first detected in Colombia, had shown signs of evading the immune response triggered by either COVID-19 vaccines or previous infection. PHE has labelled the variant “under investigation” but has not declared it a “variant of concern” – a designation that can trigger strong policy responses. “There is preliminary laboratory evidence to suggest that vaccination and previous infection may be less effective at preventing infection with (B.1.621),” it said, adding there had been 37 confirmed cases of the variant in England.
How to redefine “rare”: “..34.9 percent had received two doses..”
• In England, Hundreds Of Vaccinated People Hospitalised With Delta (AlJ)
Hundreds of fully vaccinated people in England have been hospitalised with the highly contagious Delta coronavirus variant, scientists said on Friday. In its latest COVID-19 update, Public Health England (PHE) also warned there were early signs that people who have been inoculated may be able to transmit the Delta strain as easily as those who have not received any jabs. From July 19 to August 2, 55.1 percent of the 1,467 people hospitalised with the Delta variant were unvaccinated, PHE said, while 34.9 percent – or 512 people – had received two doses. Dubbed “freedom day”, July 19 was the date England significantly eased lockdown restrictions. All vaccines in use in the United Kingdom – those produced by AstraZeneca, Moderna and Pfizer-BioNTech – require recipients to receive two doses to be fully inoculated.
About 75 percent of the UK’s adult population has received two shots to date. “As more of the population gets vaccinated, we will see a higher relative percentage of vaccinated people in hospital,” PHE said. Jenny Harries, chief executive of the UK Health Security Agency, said the hospitalisation figures showed “once again how important it is that we all come forward to receive both doses of the vaccine as soon as we are able to do so”. “Vaccination is the best tool we have in keeping ourselves and our loved ones safe from the serious disease risk COVID-19 can pose,” Harries said in a statement. “However, we must also remember that the vaccines do not eliminate all risk: it is still possible to become unwell with COVID-19 and infect others.”
“..such infection simultaneously assists in offering protection against developing variants.”
• Greater Antibody Response In Recovered COVID Patients Than Vaccinated (Fed.)
A new study has found that individuals that have previously contracted COVID-19 show a more potent antibody response than those who were solely vaccinated for the respiratory virus. Conducted by a research team at Rockefeller University in New York, the analysis found “that between a first (prime) and second (booster) shot of either the Pfizer-BioNTech or Moderna vaccine, the memory B cells of infection-naïve individuals produced antibodies that evolved increased neutralizing activity against SARS-CoV-2,” but also that “no additional increase in the potency or breadth of this activity was observed thereafter.” Meanwhile, researchers determined that not only do recovered COVID-19 patients possess neutralizing antibodies up to a year after infection, but that such infection simultaneously assists in offering protection against developing variants.
“Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection produces B-cell responses that continue to evolve for at least one year,” the study read. “During that time, memory B cells express increasingly broad and potent antibodies that are resistant to mutations found in variants of concern.” The analysis later goes on to conclude, “Memory antibodies selected over time by natural infection have greater potency and breadth than antibodies elicited by vaccination.” Moreover, the results suggest that “boosting vaccinated individuals with currently available mRNA vaccines would produce a quantitative increase in plasma neutralizing activity but not the qualitative advantage against variants obtained by vaccinating convalescent individuals.”
The study’s findings add to further mounting evidence detailing the level of protection natural immunity offers previously infected COVID-19 patients. Last month, Emory University published an extensive investigation describing the efficiency of long-term immunity against the respiratory virus. Similar discoveries have also been identified in research released by the Cleveland Clinic and the Washington University School of Medicine in St. Louis, respectively.
Every next shot is more dangerous.
• Swedish Professor Says 5 Shots of COVID Vaccine May be Necessary (SN)
While many people have bragged about being “fully vaccinated” after taking two COVID-19 jabs, a Swedish professor says that as many as five shots may be needed to combat falling immunity. “We don’t know how long the vaccine protects against serious illness and death,” said Karolinska Institute Professor Matti Sällberg. “This means that you pick the safe before the unsafe.” Numerous European countries are planning a 3rd round of COVID “booster shots” in September, and the FDA also indicated that vaccinated individuals will be given another shot in the fall. However, Sällberg suggests this probably won’t be enough and that “recurring shots” will be necessary. “After receiving the second dose, the immune response slowly subsides. Within a year, many may have lost their protection. We do not know yet, but if you get a third dose, it will be activated again,” he said. “Biology says that a fading immune response is not unlikely. Then it’s time for a third, fourth, maybe fifth dose”.
One wonders whether Sällberg holds a conflict of interest given that he is also chairman of the board at vaccine company SVF. Meanwhile, in Israel, a doctor warned that “the effectiveness of the vaccine is waning/fading out” and that “85-90% of the hospitalizations are in fully vaccinated people.” Dr. Kobi Haviv also chillingly pointed out that 95% of the patients in hospital with the most severe symptoms are vaccinated. The meme below is already coming true, and with vaccine passports seemingly on the way, people will have to keep taking recurring vaccinations simply to maintain access to basic lifestyle activities. Whether vaccine side-effects or the hassle of continually having to return for more jabs will put some people off remains to be seen.
“..both the vaxxed and non-vaxxed person walking into a restaurant, store, group, venue or workplace present the exact same risk to other people there, so how does the presentation of proof of vaccine make any difference?”
• CDC Director Makes Case Vaccination Passports are Futile (CTH)
They are just making up narratives now, and the media are not calling them out on it…. The Director of the CDC made an important admission during an interview today on CNN. CDC Director Rochelle Walensky stated the vaccine does not prevent COVID-19 infection, nor does it stop the vaccinated person from transmitting the infection or the delta variant. According to Director Walensky, the only benefit from the vaccine now is presumably that it reduces the severity of symptoms. If a vaccinated and non-vaccinated person have the same capacity to carry, shed and transmit the virus – with or without symptoms – then what difference does a vaccination passport or vaccination ID make? According to the CDC TODAY, both the vaxxed and non-vaxxed person walking into a restaurant, store, group, venue or workplace present the exact same risk to other people there, so how does the presentation of proof of vaccine make any difference?
Additionally, her entire statement makes no sense. There is no evidence that vaccinated asymptomatic carriers are asymptomatic because of the vaccine. There are likely just as many asymptomatic non-vaccinated carriers. The data shows an equally distributed infection rate regardless of vaccination rate, which is simultaneously admitted by Direcor Walensky, which, as an outcome, is an admission that undercuts the entire argument for compulsory vaccines. The reverse is also evident in the data. There are just as many vaxxed carriers who are symptomatic (ie. sick), as there are un-vaxxed carriers who are symptomatic (ie. sick). The percentage of vaxxed and non-vaxxed people hospitalized it identical to the vaxxed/non-vaxxed population around the hospital.
In regional populations with extremely high vaccination rates, the COVID infection rate continues unabated. The percentage of vaccinated people hospitalized is identical to the percentage of people vaccinated in the community. In Gibraltar, 99% of the population vaccinated; COVID infection rate climbs. In Iceland over 75% of population vaccinated; infection rate climbs. Singapore and Israel show the same thing [Data Sets Here]. So what value is the vaccination passport?
Does Fauci agree?
• White House: No More Lockdowns Of Schools Or Economy Despite Covid Rise (JTN)
The Biden White House insisted Friday that American schools and the economy will not shut down again even as COVID-19 infections rise with the new Delta variant. “We are not going back. We are not turning back the clock,” Press Secretary Jen Psaki told reporters. “This is not March 2020 or even January 2021,” she added. “We’re not going to lock down our economy or our schools because our country’s in a much stronger place than when we took office.” The promise came as some teachers unions aligned with the Democratic Party call for the school year to begin with virtual classes, not in-classroom learning.
No lockdowns in US, but the UK knows better.
• UK Draws Up Contingency Plans For ‘Firebreak’ Covid Lockdowns (iN)
The government has put contingency plans in place for further Covid-19 lockdowns should the NHS be forced back to the brink over winter, i can reveal. While No10 is confident that the vaccine rollout will prevent Covid hospitalisations rising to the levels that led to previous lockdowns, there remains concern that the NHS could be put under intense pressure from issues such as a large resurgence in patients suffering serious flu symptoms. A senior government source has told i that the Prime Minister authorised planning for “firebreak” lockdowns if a number of factors combine to push the NHS to breaking point in the autumn and winter months. There are also said to be concerns at a sharp increase in the number of NHS staff taking sick leave following 18 months fighting on the front line of the pandemic.
“The Government believes it has got to grips with the pandemic following the vaccine rollout,” said the Government advisor. “Barring a new vaccine-beating strain, fears over a rise in infections similar to that seen last autumn are actually outweighed by other issues like an NHS staffing crisis and the likely resurgence in flu infections, and other respiratory diseases. On top of Covid infections these factors could tip the NHS back to the brink and force more lockdowns.” However, the source added the Government is determined to avoid the long lockdowns the UK has endured since the pandemic struck in March 2020. = “Should more lockdowns be necessary, the plan is for them to be short, and preferably during the school holidays in late October and over Christmas. Firebreaks rather than lasting for months at a time.”
Zero covid is a really stupid idea. So, ideal for Australia.
• Australia’s ‘Covid Zero’ Days May Be Numbered (ST)
Australia’s coveted status as a haven from the pandemic could be at an end, with experts warning that a sustained Delta outbreak makes a return to “Covid zero” unlikely. After long stretches with zero local cases – what Australians once jokingly referred to as “doughnut days” – a Sydney outbreak has now grown to 4,610. Record numbers of new cases are being reported each day despite widespread lockdowns. Slowly but surely, some local authorities have shifted to talking about containing the virus rather than beating it. “Given where numbers are, given the experience of Delta overseas, we now have to live with Delta one way or another, and that is pretty obvious,” said New South Wales Premier Gladys Berejiklian. After 18 months of advocating “Covid zero”, that represents a step-change in the country’s approach.
For experts like Emma McBryde, an infectious diseases and statistical modelling expert at James Cook University, the shift in tone is a reflection of the new reality that Delta has brought. “We’re buying time, not getting back to Covid zero,” she told AFP. Like most experts she agrees that Australia’s old virus toolbox – aggressive tracing and testing, snap lockdowns and extensive travel restrictions – while less effective, is still essential to stop exponential virus spread. But, she said: “The goal now should be keeping Covid in check for long enough to get vaccinated.” Dr Tony Blakely, an epidemiologist at the University of Melbourne, echoed those comments, telling public broadcaster ABC that Australia will “probably never” get back to zero transmission.
Barring a few isolated Pacific islands and neighbouring New Zealand, few countries weathered the first 18 months of the coronavirus quite as well as Australia. As the rest of the world hunkered down, got sick and lost loved ones, Australians flocked to bars, restaurants and the beach. Occasionally, the virus jumped from hotel quarantine facilities into the community but aggressive tracing and testing, snap local lockdowns and domestic travel restrictions kept it in check. Then came Delta.
“An admitted IU student’s right to attend IU cannot be conditioned on the student waiving their rights to bodily integrity and autonomy..”
• Indiana University Students Appeal Vaccine Mandate To US Supreme Court (JTN)
First Amendment attorney Jim Bopp filed an appeal to the U.S. Supreme Court on Friday on behalf of eight Indiana University students, asking the nation’s top court to stop the university from enforcing its COVID-19 vaccine mandate. “Continuing our fight against this unconstitutional mandate is necessary to guarantee that IU students receive the fair due process they’re owed by a public university,” Bopp said in a statement sent to the media. “An admitted IU student’s right to attend IU cannot be conditioned on the student waiving their rights to bodily integrity and autonomy and to consent to medical treatment like IU has done here. The emergency application for writ of injunction was sent to Associate Supreme Court Justice Amy Coney Barrett, who is assigned to review cases coming out of the Seventh Circuit Court of Appeals.
Bopp is requesting she issue a decision by Aug. 13, 10 days before the start of IU’s fall semester Aug. 23. Indiana University announced its COVID-19 vaccine mandate May 21, outlining what it called “strong consequences” for all those who did not comply – students would have their classes canceled and email accounts cut off, the university said, and employees would be fired if they hadn’t gotten the vaccine by the start of the fall semester. The university said exemptions would be “strictly limited to a very narrow set of criteria, including medical exemptions, and documented and significant religious exemptions.” Students were told they needed to get their first dose of the vaccine by July 1 in order to be fully vaccinated by the start of school.
In response to angry calls from parents and a letter signed by the majority of Indiana’s state senators (all Republicans) expressing concerns with the mandate, IU softened its position, and began to grant all religious exemptions. But those students were told they would need to continue to wear masks, would likely be prohibited from attending certain events on campus and would be subjected to frequent testing. Then in mid-July, the university introduced an ethical exemption, allowing students and employees who don’t qualify for a medical exemption and do not want to object on religious grounds to cite personal ethics as a reason for not choosing to get the vaccine. The U.S. District Court for the Northern District of Indiana upheld the mandate in July, and a three-judge panel with the Seventh Circuit Court of Appeals also sided with IU, saying if IU students didn’t want to get the vaccine, they could go elsewhere. Bopp said his firm filed suit “to preserve students’ rights to bodily integrity and autonomy and the right to consent to medical treatment.”
The Hill labels it a “Stunning new report”. They must be the only ones who didn’t know yet.
• US Last In Health Care Among Richest Countries Despite Spending Most (Hill)
The U.S. health care system ranked last among 11 wealthy countries despite spending the highest percentage of its gross domestic product on health care, according to an analysis by the Commonwealth Fund. Researchers behind the report surveyed tens of thousands of patients and doctors in each country and used data from the Organization for Economic Cooperation and Development and the World Health Organization (WHO). The report considered 71 performance measures that fell under five categories: access to care, the care process, administrative efficiency, equity and health care outcomes. Countries analyzed in the report include Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, the United Kingdom and the U.S. Norway, the Netherlands and Australia were the top-performing countries overall, with the U.S. coming in dead last.
The U.S. ranked last on access to care, administrative efficiency, equity and health care outcomes despite spending 17 percent of GDP on health care, but came in second on the measures of care process metric. The nation performed well in rates of mammography screening and influenza vaccination for older Americans, as well as the percentage of adults who talked with their physician about nutrition, smoking and alcohol use. Half of lower-income U.S. adults in the report said costs prevented them from receiving care while just more than a quarter of high-income Americans said the same. In comparison, just 12 percent of lower-income residents in the U.K. and 7 percent with higher incomes said costs stopped them from getting care. The U.S. also had the highest infant mortality rate and lowest life expectancy at age 60 compared with other countries.
Obsessed with power.
• Dems’ Crusade Against Trump Does Real Harm To Presidency, Constitution (Fox)
The progressive crusade to bring down Donald Trump by any means necessary continues to damage the Office of the President and the Constitution’s separation of powers. New York prosecutors succeeded in subpoenaing a sitting president — and thereby interfering with his ability to carry out his duties — all for the sake of indicting a single Trump Organization official for under-reporting taxes. Now the Biden administration has inflicted even more damage on the Presidency by waiving Trump’s constitutional right to confidential communications with his closest aides. On January 23, 2021, Senate Judiciary Committee Democrats sent a letter to the Department of Justice demanding production of documents concerning meetings and communications between Trump and high-ranking Justice Department officials regarding election fraud.
House and the Senate committees subsequently followed up with subpoenas for a slew of top former Justice Department officials, such as Acting Attorney General Jeffrey Rosen, assistant attorney general Jeffrey Clark, and U.S. Attorneys in Georgia and New York. In normal times, the Justice Department would immediately reject these demands. Article II of the Constitution specifies, after all, that the President “may require the Opinion” from his principal officers “upon any Subject relating to the Duties of their respective offices.” Ever since President George Washington refused to share documents with the House about the Jay Treaty, the Executive Branch has asserted the need to keep confidential documents and information that reflect presidential decision-making and deliberation.
In Nixon v. United States, the Supreme Court recognized that the President must enjoy an executive privilege in order to receive the full and frank advice of top officials in order to effectively discharge his constitutional duties. More recently, the D.C. federal court has recognized that “history and legal precedent teach that documents from a former or an incumbent President are presumptively privileged.” The Supreme Court has only recognized an exception when a criminal defendant’s own constitutional right to information conflicts with the President’s right to confidentiality. Then—and only then—has the Court sought to balance the two competing rights by intruding only as necessary on the claim of privilege. Congress’s demands for documents and subpoenas for testimony are more far-reaching and much more destructive to the separation of powers.
While Congress has a right to investigate the events leading to the terrible riot of January 6, it does not have a right to override the constitutional prerogatives of an independent branch of government. If Congress has the right to demand presidential documents and discussions at will, it could just as easily force the Justices of the Supreme Court to reveal their deliberations about the electoral fraud cases brought after the November 3 elections, too. Imagine the howls from Capitol Hill if the Trump Justice Department had issued subpoenas to Nancy Pelosi to obtain internal documents and communications between her and her top legislative advisors about threat assessments provided in the run-up to the January 6 joint meeting of Congress.
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Support the Automatic Earth in virustime. Click at the top of the sidebars to donate with Paypal and Patreon.

Home › Forums › Debt Rattle August 7 2021