Francisco Goya Fire at night 1793-94

The 1905 SCOTUS case Jacobson v Massachusetts held that mandates can only be considered to “prevent the spread of contagious disease.”
As all studies show the shots don’t stop transmission, Covid mandates are obviously illegal.
The Miracle Vaccine Nobody Will Talk About: Covax-19

Can’t catch it well in this format, do read it. He shifts reporting of deaths by just a week, and the world looks entirely different.
Norman Fenton is Professor in Risk Information Management
@profnfenton: “Turns out that, simply by delayed reporting of deaths by 1 week, it’s inevitable a placebo will appear to reduce mortality in those who receive it compared to those who don’t..”
• Is Vaccine Efficacy A Statistical Illusion? (Fenton)
Suppose we want to examine and compare the mortality rates of the unvaccinated and vaccinated cohorts based on the data in Table 2. Figure 1 shows this comparison, and we can see that the mortality rate is consistently lower for the vaccinated than that for the unvaccinated throughout the roll out of the vaccination programme and it reduces as soon as vaccination nears population saturation at close to 100%.
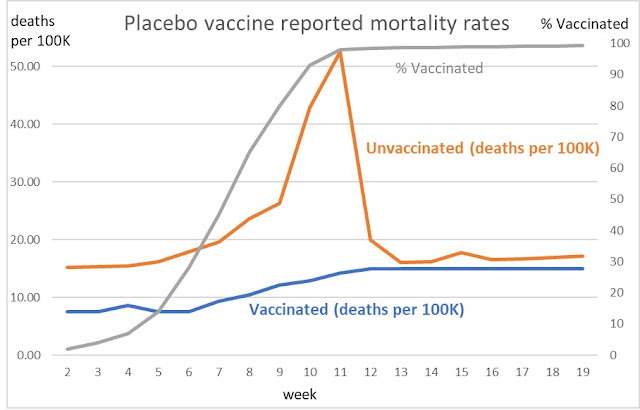
Figure 1 Reported weekly mortality rates vaccinated against unvaccinated
We might conclude that those who remain unvaccinated look to be suffering much higher levels of mortality than the vaccinated. The reporting delay therefore creates a completely artificial impression that the vaccine must be highly effective. In fact, it looks like a magic ‘cure all’ wonder drug! The fact that the mortality rate of the unvaccinated peaks when the percentage of those vaccinated peaks should ring some alarm bells that something strange is going on (unless there is independent evidence that the virus was peaking at the same time).
While the placebo vaccine example was purely hypothetical, Figure 2 shows the vaccinated against unvaccinated mortality using the data in the latest ONS report mortality in England by Covid-19 vaccination status (weeks 1 to 38)[1], complemented by NIMS vaccination survey data (up to week 27 only). Here we show other-than covid mortality to remove the virus signal.
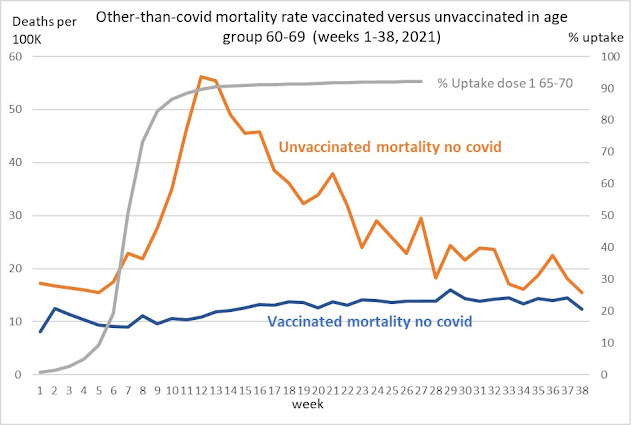
Figure 2 Reported weekly other-than covid mortality rates for vaccinated versus unvaccinated for 60-69 age group for weeks 1-38 2021
Note that we see the same features as the shifted graph in Figure 1. In other words, a perfectly reasonable explanation for what is observed here could be that there is no difference in mortality rates between vaccinated and unvaccinated and the mortality differences are simply a result of a delay in death reporting. Moreover, given we have removed covid deaths (which were only a small percentage of all-cause deaths in the reported data) we get a near identical result for non-covid mortality to that which would result if the vaccine were a placebo! Thus, we appear to have created a statistical illusion of vaccine efficacy.
If this is not a statistical illusion how is it possible that the unvaccinated are dying from non-covid causes at a higher rate than vaccinated? Also how is it possible that, at the time vaccination rates are ramped up to nearly 100% of the population, the nonvaccinated are dying from non-covid deaths at almost twice the rate of those who are vaccinated?
These same patterns are also observable in the 70-79 and 80+ age groups (with the mortality peaks for the unvaccinated appearing at different weeks because these age groups received vaccinations earlier). This strongly suggests that what we are observing is a genuine statistical illusion unexplainable by any real impact of the vaccine on mortality rates. There could, of course, be reasons other than just delays in death reporting or misclassification. For example, any systematic underestimation of the actual proportion who remain unvaccinated would lead to a higher mortality rate for unvaccinated higher than that for the vaccinated, even if the mortality rates were equal in each category.
“It can’t happen if there are no susceptible people. But it is. So there are susceptible people. How did they become susceptible when they weren’t before in any material size? We jabbed them.”
• What They Didn’t Tell You (Denninger)
This study is a bit dense — but has been peer-reviewed, and makes clear that indeed, what I hypothesized was true — and had to be, given the circumstances with Diamond Princess and elsewhere, in fact validates by scientific fact. “In summary, RTC regions like polymerase, expressed in the first stage of the viral life cycle, are highly conserved among HCoV and are preferentially targeted by T-cells in pre-pandemic and SN-HCW samples. A subset of T-cells from donors able to abort infection could cross-recognise SARS-CoV-2 and HCoV sequences at individual RTC epitopes, pointing to prior infection with HCoV as one source of pre-existing cross-reactive T-cells. ” “SN-HCW” are health-care workers who were repeatedly exposed and while they did not get sick or seroconvert “(SeroNegative)” showed very rapid response to Covid-19 from cross-reaction as a result of other coronavirus exposures.
Remember that Diamond Princess only had about 20% of the population on board that got sick despite all of them being confined together over an extended period, and even more-telling, there were multiple instances where one member of a cabin pair (husband and wife, usually) got seriously ill while the other did not only not get ill they did not test positive either. This also occurred among a couple I know early in the pandemic; one (the husband) was killed by the virus, the other (the wife) never got sick. What’s even more damning is that by May of this year about 20% of the population, according to a NEJM study that I wrote on, had seroconverted. This strongly implies that statistically everyone who could get Covid-19 and have a serious problem with already had done so.
So how is that we had a “surge” this summer and continue to see infections this fall? It can’t happen if there are no susceptible people. But it is. So there are susceptible people. How did they become susceptible when they weren’t before in any material size? We jabbed them. The CDC and hospitals do not count someone who gets Covid before 2 weeks after their last jab as “vaccinated.” So if you have a cycle of 28 days from first to second from the first jab to a period of time six weeks later if you get Covid-19 you’re considered “unvaccinated.” Every place where we’ve had very high vaccination uptake as the uptake occurred we have seen material spikes in infection contemporary with the jabs, even out of regular season with normal respiratory viral patterns.
Why? The reasonable hypothesis is that the jabs are destroying pre-existing resistance that formerly was sufficient to prevent significant, seroconverting infections in about 8 out of 10 people, but post-jab that resistance is suppressed either temporarily or permanently and thus they are able to get significantly infected.
‘No one’s saying that the information [about ivermectin’s efficacy] has been deliberately hidden away while millions of people have died’
• New Pfizer Drug and Ivermectin (Campbell)
Lots of Pfizer ads? How many millions on a yearly basis?
• COVID-19 Vaccine-Myocarditis Paper To Be Permanently Removed: Elsevier (RW)
A paper claiming that cases of myocarditis spiked after teenagers began receiving COVID-19 vaccines that earned a “temporary removal” earlier this month will be permanently removed, according to a publisher at Elsevier. As we reported last week, the article, “A Report on Myocarditis Adverse Events in the U.S. Vaccine Adverse Events Reporting System (VAERS) in Association with COVID-19 Injectable Biological Products,” was published in Current Problems in Cardiology on October 1. Sometime between then and October 17, the article was stamped “TEMPORARY REMOVAL” without explanation other than Elsevier’s boilerplate notice in such cases:
“The Publisher regrets that this article has been temporarily removed. A replacement will appear as soon as possible in which the reason for the removal of the article will be specified, or the article will be reinstated. The full Elsevier Policy on Article Withdrawal can be found at http://www.elsevier.com/locate/withdrawalpolicy.” In an email to co-author Peter McCullough, Elsevier publisher Diana Goetz said that “the journal is not willing to publish the paper.” Here’s the entire email:
Goetz did not respond to requests for comment from Retraction Watch about whether a retraction notice explaining the move would appear. Elsevier’s policy on such matters has changed slightly over the years, but the central lack of transparency on their “withdrawals” has been the subject of our coverage since 2013. Jessica Rose, the other author of the paper, told Retraction Watch: “We are very motivated to get the information in our paper to the public: pediatricians, parents and policy-makers alike. This is why we decided to publish in the first place. It is extremely frustrating for us to face such censorship when professionals are in need of scientific data and discourse on the subject of myocarditis in children in these very strange times.” Rose’s affiliation on the removed version of the paper is the Institute of Pure and Applied Knowledge’s Public Health Policy Initiative, and McCullough’s is the Truth for Health Foundation in Tucson.
As we noted in our previous post, IPAK is “..a group that has been critical of vaccines and of the response to COVID-19 and has funded one study that was retracted earlier this year… Last month, Baylor Scott & White obtained a restraining order against McCullough — whom Medscape says “has promoted the use of therapies seen as unproven for the treatment of COVID-19 and has questioned the effectiveness of COVID-19 vaccines” — for continuing to refer to an affiliation with the health care institution despite a separation agreement. “Since the Baylor suit, the Texas A&M College of Medicine, and the Texas Christian University (TCU) and University of North Texas Health Science Center (UNTHSC) School of Medicine have both removed McCullough from their faculties,” Medscape reported at the time.”
Variants of variants.
• Delta Variant Displays Moderate Resistance To Neutralizing Antibodies (bioRxiv)
The SARS-CoV-2 B.1.617 lineage variants, Kappa (B.1.617.1) and Delta (B.1.617.2, AY) emerged during the second wave of infections in India, but the Delta variants have become dominant worldwide and continue to evolve. The spike proteins of B.1.617.1, B.1.617.2, and AY.1 variants have several substitutions in the receptor binding domain (RBD), including L452R+E484Q, L452R+T478K, and K417N+L452R+T478K, respectively, that could potentially reduce effectiveness of therapeutic antibodies and current vaccines. Here we compared B.1.617 variants, and their single and double RBD substitutions for resistance to neutralization by convalescent sera, mRNA vaccine-elicited sera, and therapeutic neutralizing antibodies using a pseudovirus neutralization assay.
Pseudoviruses with the B.1.617.1, B.1.617.2, and AY.1 spike showed a modest 1.5 to 4.4-fold reduction in neutralization titer by convalescent sera and vaccine-elicited sera. In comparison, similar modest reductions were also observed for pseudoviruses with C.37, P.1, R.1, and B.1.526 spikes, but seven- and sixteen-fold reduction for vaccine-elicited and convalescent sera, respectively, was seen for pseudoviruses with the B.1.351 spike. Four of twenty-three therapeutic neutralizing antibodies showed either complete or partial loss of neutralization against B.1.617.2 pseudoviruses due to the L452R substitution, whereas six of twenty-three therapeutic neutralizing antibodies showed either complete or partial loss of neutralization against B.1.617.1 pseudoviruses due to either the E484Q or L452R substitution.
Against AY.1 pseudoviruses, the L452R and K417N substitutions accounted for the loss of neutralization by four antibodies and one antibody, respectively, whereas one antibody lost potency that could not be fully accounted for by a single RBD substitution. The modest resistance of B.1.617 variants to vaccine-elicited sera suggest that current mRNA-based vaccines will likely remain effective in protecting against B.1.617 variants, but the therapeutic antibodies need to be carefully selected based on their resistance profiles. Finally, the spike proteins of B.1.617 variants are more efficiently cleaved due to the P681R substitution, and the spike of Delta variants exhibited greater sensitivity to soluble ACE2 neutralization, as well as fusogenic activity, which may contribute to enhanced spread of Delta variants.
Hard to speak in clear terms when you’re scientists, but:
“We observed no difference in [..] odds of in-hospital death between vaccinated and unvaccinated patients.”
Dr Anthony Hinton: “Norway Study Finds ZERO Vaccine Effectiveness Against Death for Covid Hospital Patients. The Pfizer trial never made this claim they only claimed symptom reduction.”
• Patient Trajectories Among Hospitalised Covid-19 Patients (medRxiv)
Objectives With most of the Norwegian population vaccinated against COVID-19, an increasing number and proportion of COVID-19 related hospitalisations are occurring among vaccinated patients. To support patient management and capacity planning in hospitals, we estimated the length of stay (LoS) in hospital and odds of intensive care (ICU) admission and in-hospital mortality among COVID-19 patients ≥18 years who had been vaccinated with an mRNA vaccine, compared to unvaccinated patients.
Methods Using national registry data, we conducted a cohort study on SARS-CoV-2 positive patients hospitalised in Norway between 1 February and 30 September 2021, with COVID-19 as the main cause of hospitalisation. We used a Cox proportional hazards model to examine the association between vaccination status and LoS. We used logistic regression to examine the association between vaccination status and ICU admission and in-hospital mortality.
Results We included 2,361 patients, including 70 (3%) partially vaccinated and 183 (8%) fully vaccinated. Fully vaccinated patients 18–79 years had a shorter LoS in hospital overall (adjusted hazard ratio for discharge: 1.35, 95%CI: 1.07–1.72), and lower odds of ICU admission (adjusted odds ratio: 0.57, 95%CI: 0.33–0.96). Similar estimates were observed when collectively analysing partially and fully vaccinated patients. We observed no difference in the LoS for patients not admitted to ICU, nor odds of in-hospital death between vaccinated and unvaccinated patients.
Conclusions Vaccinated patients hospitalised with COVID-19 in Norway have a shorter LoS and lower odds of ICU admission than unvaccinated patients. These findings can support patient management and ongoing capacity planning in hospitals.
Axios: “A reckoning is hitting news organizations for years-old coverage of the 2017 Steele dossier, after the document’s primary source was charged with lying to the FBI.”
• The Media’s Epic Fail On The Steele Dossier (Axios)
A reckoning is hitting news organizations for years-old coverage of the 2017 Steele dossier, after the document’s primary source was charged with lying to the FBI. Why it matters: It’s one of the most egregious journalistic errors in modern history, and the media’s response to its own mistakes has so far been tepid. Outsized coverage of the unvetted document drove a media frenzy at the start of Donald Trump’s presidency that helped drive a narrative of collusion between former President Trump and Russia. It also helped drive an even bigger wedge between former President Trump and the press at the very beginning of his presidency.
Driving the news: In wake of the key source’s arrest and further reporting on the situation, The Washington Post on Friday corrected and removed large portions of two articles. To The Post’s credit, its media critic, Erik Wemple, has written at length about the mistakes made by The Post and other media outlets in their coverage of the dossier. BuzzFeed News, which made waves in 2017 by publishing the entire dossier, says it has no plans to take the document down. It’s still online, accompanied by a note that says “The allegations are unverified, and the report contains errors.” Ben Smith, who was BuzzFeed’s editor-in-chief at the time and is now a media columnist at The New York Times, told Axios, “My view on the logic of publishing hasn’t changed.”
BuzzFeed defended the decision in a 2018 lawsuit by arguing that because the FBI opened an investigation into the Trump campaign’s ties to Russia, the dossier itself was newsworthy, whatever the merits of its contents turned out to be. It won that case. Other outlets that gave the document outsized coverage have so far been less forthcoming. CNN and MSNBC did not respond to requests for comment about whether they planned to revisit or correct any of their coverage around the dossier. Mother Jones Washington bureau chief David Corn began reporting about the dossier prior to the 2016 election. Asked by Wemple whether he planned to correct the record, Corn said,” My priority has been to deal with the much larger topic of Russia’s undisputed attack and Trump’s undisputed collaboration with Moscow’s cover-up.”
The Wall Street Journal told Axios, “We’re aware of the serious questions raised by the allegations and continue to report and to follow the investigation closely.” Axios was among the outlets that did not publish the dossier or original reporting based on its contents. What to watch: The Steele screwup will undoubtedly cause an even bigger rift in trust between Democrats and Republicans.
“It’s CNN who is involved in vigilante justice. It’s The New Yorker that’s guilty of vigilante justice.”
• Alan Dershowitz: Kyle Rittenhouse ‘Should Be Acquitted’ And Sue Media (JTN)
Alan Dershowitz, the famed Harvard law professor emeritus, said Kyle Rittenhouse “should be acquitted” of injuring a man and killing two others in Kenosha, Wis., and sue media outlets that are claiming he’s guilty of vigilante justice. “If I were a juror, I would vote that there was reasonable doubt [and] that he did act in self-defense,” Dershowitz told Newsmax on Saturday.”Then he’ll bring lawsuits, and that’s the way to answer… vigilante justice is what CNN is doing, not what a 17-year-old kid under pressure may have done right or wrong. It’s CNN who is involved in vigilante justice. It’s The New Yorker that’s guilty of vigilante justice.”
Dershowitz referenced then-Kentucky high school student Nicholas Sandmann and how he sued and settled with CNN and The Washington Post for defamation as they accused him of being racist following viral videos of an encounter he had with a Native American activist in Washington, D.C. “The idea is to make the media accountable for deliberate and willful lies,” he said. Dershowitz added that “the left-wing media … is attacking this judge for trying to be fair. They want an outcome. They want a result and if they don’t get their results and you know this seeps through to the jury, and I worry that the jury could be influenced by the fear that if they vote to acquit, they’ll be called racist and they’ll be attacked.”
Judge: “I have been wrestling with this statute with, I’d hate to count the hours I’ve put into it, I’m still trying to figure out what it says, what’s prohibited. I have a legal education.”
• Was Rittenhouse’s Possession of the AR-15 Unlawful? (Turley)
In covering the motions hearing last week in the trial of Kyle Rittenhouse, I noted a surprising comment from Judge Bruce Schroeder that he had “spent hours” with the Wisconsin gun law and could not state with certainty what it means in this case. The statement could effectively knock out the misdemeanor gun possession count — the one count that could still be in play for the jury after the prosecution’s case on the more serious offense appeared to collapse in court. A close examination of that provision reveals ample reason to question not just its meaning but its application to this case. The unlawful possession of the gun has been a prominent fact cited not only by the prosecutors but the press. At trial, however, prosecutor Thomas Binger at points seemed to be learning the governing law from Rittenhouse.
For example, he pressed Rittenhouse on why he did not just purchase a handgun rather than an AR-15. Rittenhouse replied he could not possess a hand gun at his age. Binger then asked in apparent disbelief that the law allowed him to have an AR-15 but not a handgun and Rittenhouse said yes. Binger then moved on after seemingly drawing out a point for the defenseThe exchange was all the more baffling because it drew attention to the fact that one of Binger’s alleged “victims” was an adult named Gaige Grosskreutz who also decided to bring a handgun to the protests and pointed his .40 caliber Glock at the head of Rittenhouse when he was shot in the arm. However, the most damaging moment came outside of the presence of the jury when the judge drilled down on the law.
He told the prosecutors “I have been wrestling with this statute with, I’d hate to count the hours I’ve put into it, I’m still trying to figure out what it says, what’s prohibited. I have a legal education.” He added that he failed to understand how an “ordinary citizen” could understand what is illegal. It is hard to understand how the count could be given to the jury without a clear understanding of what it means. It is also hard to instruct a jury on an ambiguous statute. Criminal laws are supposed to be interpreted narrowly. It is called the “rule of lenity” and has been around in the English system for centuries. For example, in 1547, the court was faced with a law making it a felony to steal “Horses, Geldings or Mares.” Given the use of plural nouns, the court ruled that it did not apply to stealing just one horse.
The problem with the Wisconsin statute is not a problem of pluralization but definition. It is not clear that the statute actually bars possession by Rittenhouse. Indeed, it may come down to the length of Rittenhouse’s weapon and the prosecutors never bothered to measure it and place it into evidence. In Wisconsin, minors cannot possess short-barreled rifles under Section 941.28. Putting aside the failure to put evidence into the record to claim such a short length, it does not appear to be the case here. Rittenhouse used a Smith & Wesson MP-15 with an advertised barrel length of 16 inches and the overall length is 36.9 inches. That is not a short barrel.

Support the Automatic Earth in virustime; donate with Paypal, Bitcoin and Patreon.