

Thomas Cole The Course of Empire – Desolation 1836

A longtime friend in the US, an emeritus professor, sent me an email recently with a mail exchange between his wife and sister, in which the latter called the Automatic Earth a “conservative website” (first time I heard that one), and said: “When they never cite a source, I call the whole diatribe bullshit. Show me some real, creditable, data, and then we can talk.”
This was in reaction to my September 20 article The Vaccines Kill Many More People Than They Save about Steve Kirsch and his research. I replied -of course- that Kirsch is very meticulous about his sources. And we have more where that came from.
ScienceDirect, an publication by Elsevier, one of the world’s biggest publishers of scientific papers (500,000 a year), has started a special section on Covid named Toxicology Reports: COVID-19 Pandemic: Health impact and Novel research. A recent report in that section is entitled Why Are We Vaccinating Children Against Covid-19?
The authors conclude that there have been at most 35,000 Covid deaths in the US so far, not over 600,000. Because “94 % of the reported deaths had multiple comorbidities”. What could well be over 600,000 is the number of Covid vaccine deaths. Registered VAERS vaccine deaths currently are 14,925.
Basically, they leave nothing standing of the mass vaccination, the vaccine passports, QR codes, none of it. They call the vaccines “treatments” because they don’t comply with the 2000 definition of a vaccine from the U.S. Patent Office, which states “The immune response produced by a vaccine must be more than merely some immune response but must be protective”. They also state that even in the high-risk group of people over 65, the vaccines kill 5 times more people than Covid.
The reason I come back to this -again- is that reports like this, critical of official vaccine policies, and certainly not just in the US, receive no media attention at all. Crickets. It doesn’t even matter who publishes them. You can be the biggest medical publishing house, or the biggest medical journal, the only thing that counts is toeing the party line.
My question is at what point do the politicians and journalists that run this show cease to be accomplices to murder? Because that is what is happening here. And there will be a moment when people find this out. What will they all have to say then?
I can only give you some bits and pieces from the report, it’s exhaustive, and has more sources than any one person could probably read in a whole year. The conclusion:“It is unclear why this mass inoculation for all groups is being done, being allowed, and being promoted.”
Now, I understand that medical researchers must be conservative in their statements, but I would venture that if they are right, that even in the age group at the highest risk, the chance of dying from the vaccines is 5 times higher than dying of Covid, 65+, the appropriate term is not “unclear”, but “criminal”.
Robert W Malone, MD read the report and says: “In summary, the value of these COVID-19 inoculations is not obvious from a cost-benefit perspective for the most vulnerable age demographic, and is not obvious from any perspective for the least vulnerable age demographic.”
“Thus, our extremely conservative estimate for risk-benefit ratio is about 5/1. In plain English, people in the 65+ demographic are five times as likely to die from the inoculation as from COVID-19 under the most favorable assumptions! ”
Why Are We Vaccinating Children Against Covid-19?
1. Introduction
A vaccine is legally defined as any substance designed to be administered to a human being for the prevention of one or more diseases. For example, a January 2000 patent application that defined vaccines as “compositions or mixtures that when introduced into the circulatory system of an animal will evoke a protective response to a pathogen.” was rejected by the U.S. Patent Office because “The immune response produced by a vaccine must be more than merely some immune response but must be protective”. As noted in the previous Office Action, the art recognizes the term “vaccine” to be a compound which prevents infection”. In the remainder of this article, we use the term ‘inoculated’ rather than vaccinated, because the injected material in the present COVID-19 inoculations prevents neither viral infection nor transmission. Since its main function in practice appears to be symptom suppression, it is operationally a “treatment”.
2. Background
2.1. Pandemic history
[..] in the USA, nearly 600,000 deaths have been officially attributed to COVID-19. Almost 5,000 deaths following inoculation have been reported to VAERS by late May 2021; specifically, “Over 285 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through May 24, 2021. During this time, VAERS received 4,863 reports of death (0.0017 %) among people who received a COVID-19 vaccine.” [3] (the Vaccine Adverse Events Reporting System (VAERS) is a passive surveillance system managed jointly by the CDC and FDA. Historically, VAERS has been shown to report about 1% of actual vaccine/inoculation adverse events. [..] By mid-June, deaths following COVID-19 inoculations had reached the ˜6000 levels. [Note: 14,925 today]
[..] By the end of May 2021, the official CDC death count attributed to COVID-19 was approaching 600,000, as stated previously. This number has been disputed for many reasons. First, before COVID-19 testing began, or in the absence of testing, after it was available, the diagnosis of COVID-19 (in the USA) could be made by the presumption of the healthcare practitioner that COVID-19 existed. Second, after testing began, the main diagnostic used was the RT-PCR test. This test was done at very high amplification cycles, ranging up to 45. In this range, very high numbers of false positives are possible.
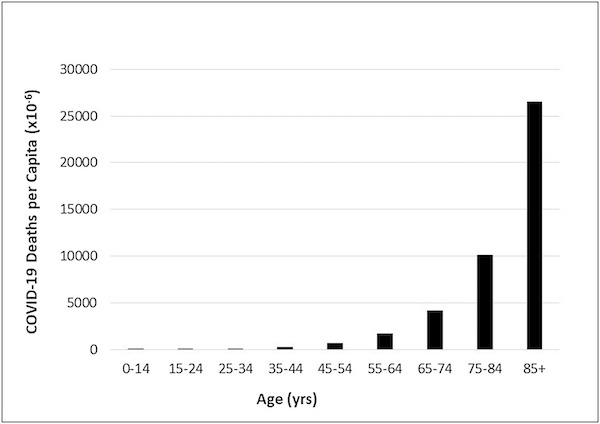
Fig. 1. COVID-19 Deaths per capita by age in the United States (as of Jun 5, 2021). Population-based on U.S. CDC WONDER Bridge-Race Population Estimate 2019. Data obtained from https://wonder.cdc.gov/bridged-race-v2019.html on 6/15/2021. Provisional COVID-19 deaths based on CDC data provided by the National Center for Health Statistics for the period 1/1/2020 – 6/5/2021. Data obtained from https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-by-Sex-and-Age/9bhg-hcku on 6/10/2021.
Third, most deaths attributed to COVID-19 were elderly with high comorbidities. As we showed in a previous study, attribution of death to one of many possible comorbidities or especially toxic exposures in combinations [23] is highly arbitrary and can be viewed as a political decision more than a medical decision. For over 5 % of these deaths, COVID-19 was the only cause mentioned on the death certificate. For deaths with conditions or causes in addition to COVID-19, on average, there were 4.0 additional conditions or causes per death. These deaths with comorbidities could equally have been ascribed to any of the comorbidities. Thus, the actual number of COVID-19-based deaths in the USA may have been on the order of 35,000 or less, characteristic of a mild flu season.
Even the 35,000 deaths may be an overestimate. Comorbidities were based on the clinical definition of specific diseases, using threshold biomarker levels and relevant symptoms for the disease(s) of interest. But many people have what are known as pre-clinical conditions. The biomarkers have not reached the threshold level for official disease diagnosis, but their abnormality reflects some degree of underlying dysfunction. The immune system response (including pre-clinical conditions) to the COVID-19 viral trigger should not be expected to be the same as the response of a healthy immune system. If pre-clinical conditions had been taken into account and coupled with the false positives as well, the CDC estimate of 94 % misdiagnosis would be substantially higher.
4. Discussion
It is becoming clear that the central ingredient of the injection, the recipe for the spike protein, will produce a product that can have three effects. Two of the three occur with the production of antibodies to the spike protein. These antibodies could allegedly offer protection against the virus (although with all the “breakthrough” cases reported, that is questionable), or could suppress serious symptoms to some extent. They could also cross-react with human tissue antigen, leading to potential autoimmune effects. The third occurs when the injected material enters the bloodstream and circulates widely, which is enabled by the highly vascular injection site and the use of the PEG-2000 coating.
This allows spike protein to be manufactured/expressed in endothelial cells at any location in the body, both activating platelets to cause clotting and causing vascular damage. It is difficult to believe this effect is unknown to the manufacturer, and in any case, has been demonstrated in myriad locations in the body using VAERS data. There appears to be modest benefit from the inoculations to the elderly population most at risk, no benefit to the younger population not at risk, and much potential for harm from the inoculations to both populations.
It is unclear why this mass inoculation for all groups is being done, being allowed, and being promoted.
5. Overall conclusions
[..] Adequate safety testing of the COVID-19 inoculations would have provided a distribution of the outcomes to be expected from ‘lighting the match’. Since adequate testing was not performed, we have no idea how many combustible materials are on the floor, and what the expected outcomes will be from ‘lighting the match’. The injection goes two steps further than the wild virus because 1) it contains the instructions for making the spike protein, which several experiments are showing can cause vascular and other forms of damage, and 2) it bypasses many front-line defenses of the innate immune system to enter the bloodstream directly in part. Unlike the virus example, the injection ensures there will always be some combustible materials on the floor, even if there are no other toxic exposures or behaviors.
In other words, the spike protein and the surrounding LNP are toxins with the potential to cause myriad short-, mid-, and long-term adverse health effects even in the absence of other contributing factors! Where and when these effects occur will depend on the biodistribution of the injected material. Pfizer’s own biodistribution studies have shown the injected material can be found in myriad critical organs throughout the body, leading to the possibility of multi-organ failure. And these studies were from a single injection. Multiple injections and booster shots may have cumulative effects on organ distributions of inoculant! The COVID-19 reported deaths are people who died with COVID-19, not necessarily from COVID-19. Likewise, the VAERS deaths are people who have died following inoculation, not necessarily from inoculation.
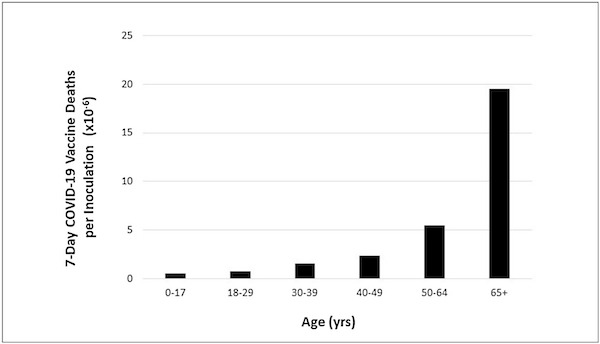
Fig. 2. Post-inoculation deaths per dose of inoculant. 7-day COVID-19 vaccine deaths per inoculation by age in the United States (as of 5/28/2021). Data shown includes the total number of all deaths up to 7 days after receiving the vaccine for both those administered 1 dose and the complete series of doses by age in the United States as of 5/28/2021 reported in VAERS (updated on 5/28/2021). COVID-19 Vaccinations (Inoculations) based on CDC data provided by ISSInfo up thru 5/28/2021. Data obtained from https://data.cdc.gov/Vaccinations/COVID-19-Vaccination-Demographics-in-the-United-St/km4m-vcsb on 6/10/2021. COVID-19 Vaccinations Deaths based on CDC WONDER VAERS Database as of 5/28/2021, obtained from https://wonder.cdc.gov/controller/datarequest/D8;jsessionid=4B5522C8D1DA68F1A364646B0DA5 on 6/9/2021.
As stated before, CDC showed that 94 % of the reported deaths had multiple comorbidities, thereby reducing the CDC’s numbers attributed strictly to COVID-19 to about 35,000 for all age groups. Given the number of high false positives from the high amplification cycle PCR tests, and the willingness of healthcare professionals to attribute death to COVID-19 in the absence of tests or sometimes even with negative PCR tests, this 35,000 number is probably highly inflated as well. On the latter issue, both Virginia Stoner [85] and Jessica Rose [86] have shown independently that the deaths following inoculation are not coincidental and are strongly related to inoculation through strong clustering around the time of injection. Our independent analyses of the VAERS database reported in Appendix 1 confirmed these clustering findings.
Additionally, VAERS historically has under-reported adverse events by about two orders-of-magnitude, so COVID-19 inoculation deaths in the short-term could be in the hundreds of thousands for the USA for the period mid-December 2020 to the end of May 2021, potentially swamping the real COVID-19 deaths. Finally, the VAERS deaths reported so far are for the very short term. We have no idea what the death numbers will be in the intermediate and long-term; the clinical trials did not test for those. The clinical trials used a non-representative younger and healthier sample to get EUA for the injection. Following EUA, the mass inoculations were administered to the very sick (and first responders) initially, and many died quite rapidly. However, because the elderly who died following COVID-19 inoculation were very frail with multiple comorbidities, their deaths could easily be attributed to causes other than the injection (as should have been the case for COVID-19 deaths as well).
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Support the Automatic Earth in virustime. Donate with Paypal, Bitcoin and Patreon.
