The FDA. the U.S. Food and Drug Administration, announced on Monday that it gave full approval to a vaccine. But it didn’t. Or rather, it did, but the approval is for a vaccine that doesn’t exist. Or rather, it exists, but it’s not being produced. Or rather, it’s being produced, but under different names and with different legal statuses.
The FDA is playing a game with Americans, in order to get them to submit to being vaccinated. And this has to stop. No more. The role of the FDA is to protect people, not cajole them into politically desired but illegal actions. Below are 3 -bullet points of- articles about the (non-) approval. One from Peter Doshi, senior editor at The BMJ, and a powerful foe to the FDA, one from Robert Kennedy jr, and one from Jill Malone, wife of Dr. Robert Malone.
But first, yet another lie -BIG, not noble- from Anthony Fauci, as told to Anderson Cooper. There is no approval for “the Pfizer product”, and Fauci knows that very well. Or rather, there is approval for a Pfizer product that is not available to anyone. And that should never have been approved the way it was in the first place, but that’s another story. Still, Fauci said it.
In theory, if he were called on it (but of course he won’t be by any reporter he talks to), he could say that the products are the same anyway. But he won’t say that, because he realizes full well that they have different legal statuses; they are “legally distinct” in the words of the FDA. So Fauci can’t say they are the same. Even if it’s just a matter of a different label on a vial.
Yes, it sounds crazy, but that’s the legal labyrinth the FDA and Pfizer have negotiated themselves into. Why? Kennedy says it best: Pfizer is unlikely to allow any American to take a Comirnaty vaccine until it can somehow arrange immunity for this product..
And: “If it says “Comirnaty,” it’s a licensed product. If it says “Pfizer-BioNTech,” it’s an experimental product, and under 21 U.S. Code 360bbb, you have the right to refuse. If it comes from Moderna or Johnson & Johnson (marketed as Janssen), you have the right to refuse. [..] If it doesn’t say Comirnaty, you have not been offered an approved vaccine.”
Jill Malone: The vaccine that is likely to be supplied for some time, WILL BE THE Pfizer – EUA vaccine. So any mandates based on full approval are meaningless.
“There was some poll that showed about 30% of people who are not anti-vax, they were just waiting to get what they felt was the real final stamp of approval, which we just got today with the Pfizer product.” He continued, “And those 30% are saying when that occurs, they will feel very, very comfortable about getting vaccinated. So right away, you’re talking about 30%. I hope they come through with what the survey said.”
[..] “They’re going to give a lot of incentive and backing for a lot of institutions and organizations and places of employment to mandate, and that could be colleges, university, the military, organizations that employ a lot of people, some of the big corporations are going to say if you want to work for us in person, you’ve got to be there and get vaccinated.”
[..] “I know I respect people’s freedom, but when you’re talking about a public health crisis that we’ve been going through for well over a year and a half, the time has come. Enough is enough. We’ve just got to get people vaccinated.” “If we keep lingering without getting those people vaccinated that should be vaccinated, this thing could linger on, leading to the development of another variant which could complicate things.”
On 28 July 2021, Pfizer and BioNTech posted updated results for their ongoing phase 3 covid-19 vaccine trial. The preprint came almost a year to the day after the historical trial commenced, and nearly four months since the companies announced vaccine efficacy estimates “up to six months.” But you won’t find 10 month follow-up data here.
While the preprint is new, the results it contains aren’t particularly up to date. In fact, the paper is based on the same data cut-off date (13 March 2021) as the 1 April press release, and its topline efficacy result is identical: 91.3% (95% CI 89.0 to 93.2) vaccine efficacy against symptomatic covid-19 through “up to six months of follow-up.”
[..] the recent reports from Israel’s Ministry of Health caught my eye. In early July, they reported that efficacy against infection and symptomatic disease “fell to 64%.” By late July it had fallen to 39% where Delta is the dominant strain. This is very low. For context, the FDA’s expectation is of “at least 50%” efficacy for any approvable vaccine.
[..] evidence of waning immunity was already visible in the data by the 13 March 2021 data cut-off… And it’s hard to imagine how the Delta variant could play a real role here, for 77% of trial participants were from the United States, where Delta was not established until months after data cut-off.
[..] Despite the reference to “six month safety and efficacy” in the preprint’s title, the paper only reports on vaccine efficacy “up to six months,” but not from six months. This is not semantics, as it turns out only 7% of trial participants actually reached six months of blinded follow-up (“8% of BNT162b2 recipients and 6% of placebo recipients had ≥6 months follow-up post-dose 2.”) So despite this preprint appearing a year after the trial began, it provides no data on vaccine efficacy past six months, which is the period Israel says vaccine efficacy has dropped to 39%.
[..] —a total of three covid-19 related deaths (one on vaccine, two on placebo). There were 29 total deaths during blinded follow-up (15 in the vaccine arm; 14 in placebo). The crucial question, however, is whether the waning efficacy seen in the primary endpoint data also applies to the vaccine’s efficacy against severe disease.
[..] here we are, with FDA reportedly on the verge of granting a marketing license 13 months into the still ongoing, two year pivotal trial, with no reported data past 13 March 2021, unclear efficacy after six months due to unblinding, evidence of waning protection irrespective of the Delta variant, and limited reporting of safety data.
Robert F. Kennedy, Jr. and Meryl Nass, M.D. at childrenshealthdefense.org.
Monday, the U.S. Food and Drug Administration (FDA) approved a biologics license application for the Pfizer Comirnaty vaccine. The press reported that vaccine mandates are now legal for military, healthcare workers, college students and employees in many industries. New York City Mayor Bill de Blasio has now required the vaccine for all teachers and school staff. The Pentagon is proceeding with its mandate for all military service members.
[..] First, the FDA acknowledges that while Pfizer has “insufficient stocks” of the newly licensed Comirnaty vaccine available, there is “a significant amount” of the Pfizer-BioNTech COVID vaccine — produced under Emergency Use Authorization (EUA) — still available for use. The FDA decrees that the Pfizer-BioNTech vaccine under the EUA should remain unlicensed but can be used “interchangeably” (page 2, footnote 8) with the newly licensed Comirnaty product. Second, the FDA pointed out that the licensed Pfizer Comirnaty vaccine and the existing, EUA Pfizer vaccine are “legally distinct,” but proclaims that their differences do not “impact safety or effectiveness.”
[..] EUA products are experimental under U.S. law. Both the Nuremberg Code and federal regulations provide that no one can force a human being to participate in this experiment. Under 21 U.S. Code Sec.360bbb-3(e)(1)(A)(ii)(III), “authorization for medical products for use in emergencies,” it is unlawful to deny someone a job or an education because they refuse to be an experimental subject. Instead, potential recipients have an absolute right to refuse EUA vaccines.
U.S. laws, however, permit employers and schools to require students and workers to take licensed vaccines. EUA-approved COVID vaccines have an extraordinary liability shield under the 2005 Public Readiness and Preparedness Act. [..] At least for the moment, the Pfizer Comirnaty vaccine has no liability shield. Vials of the branded product, which say “Comirnaty” on the label, are subject to the same product liability laws as other U.S. products.
When the Centers for Disease Control and Prevention’s (CDC) Advisory Committee for Immunization Practices places a vaccine on the mandatory schedule, a childhood vaccine benefits from a generous retinue of liability protections. But licensed adult vaccines, including the new Comirnaty, do not enjoy any liability shield. Just as with Ford’s exploding Pinto, or Monsanto’s herbicide Roundup, people injured by the Comirnaty vaccine could potentially sue for damages. And because adults injured by the vaccine will be able to show that the manufacturer knew of the problems with the product, jury awards could be astronomical.
Pfizer is therefore unlikely to allow any American to take a Comirnaty vaccine until it can somehow arrange immunity for this product.
[..] the FDA’s acknowledgement in its approval letter that there are insufficient stocks of the licensed Comirnaty, but an abundant supply of the EUA Pfizer BioNTech jab, exposes the “approval” as a cynical scheme to encourage businesses and schools to impose illegal jab mandates. The FDA’s clear motivation is to enable Pfizer to quickly unload inventories of a vaccine that science and the Vaccine Adverse Events Reporting System have exposed as unreasonably dangerous, and that the Delta variant has rendered obsolete.
Americans, told that the Pfizer COVID vaccine is now licensed, will understandably assume COVID vaccine mandates are lawful. But only EUA-authorized vaccines, for which no one has any real liability, will be available during the next few weeks when many school mandate deadlines occur. [..] While the media has trumpeted that the FDA has approved COVID vaccines, the FDA has not approved the Pfizer BioNTech vaccines, nor any COVID vaccines for the 12- to 15-year age group, nor any booster doses for anyone.
And the FDA has not licensed any Moderna vaccine, nor any vaccine from Johnson & Johnson — so the vast majority, if not all, of vaccines available in the U.S. remain unlicensed EUA products.
Here’s what you need to know when somebody orders you to get the vaccine: Ask to see the vial. If it says “Comirnaty,” it’s a licensed product. If it says “Pfizer-BioNTech,” it’s an experimental product, and under 21 U.S. Code 360bbb, you have the right to refuse. If it comes from Moderna or Johnson & Johnson (marketed as Janssen), you have the right to refuse. The FDA is playing bait and switch with the American public — but we don’t have to play along. If it doesn’t say Comirnaty, you have not been offered an approved vaccine..
FDA Pfizer authorization (Comirnaty): Key points to consider and discuss.
These points are an aggregate of many minds, including Dr. Robert Malone. 23 Aug 2021
General talking points
• Why mandates if herd immunity isn’t possible?
• What happens 8 months after boosters?
• What’s the plan for the next variant?
• Why we’re messing with vaccine injury liability if the vaccines are safe and effective?
There are now TWO LEGALLY distinct (Pfizer vs. BionTech), but otherwise identical products, based on two FDA letters, as well as a press release. The analysis of these FDA products below is preliminary and subject to change.
Letter to Pfizer
https://www.fda.gov/media/150386/download
• DOES NOT GIVE FULL APPROVAL
• Extends EUA to allow supply of current Pfizer under EUA because limited supply of BioNTech version.
• “The products are legally distinct with certain differences that do not impact safety or effectiveness. (page 2, Pfizer letter) [..] here FDA quietly admits that the licensed Pfizer vaccine and the authorized Pfizer vaccine are identical with regard to safety/efficacy, but they are “legally distinct.” That’s code for one has manufacturer liability, while the other doesn’t. It is also code for “we don’t want to impose a mandate on the EUA product cause it is illegal, but we can probably get away with a mandate on the licensed product.”
[..] yes, we licensed the vaccine, but…there is a lot of the old vaccine out there, actually “a significant amount” and this amount will be considered an EUA and will continue to be used. Now, why would they do that? Why specify that identical versions of the product will be legally different? Because they need the license to impose the mandates. But they need the EUA to evade liability.
Along with the license comes liability for the manufacturer. (While all EUA products were given a liability shield.) the feds want us to THINK the vaccine we are receiving is licensed, which will make people submit because they think it can now be mandated , but instead we are almost certain to receive the EUA vials instead, to save Pfizer’s behind.
“On August 23, 2021, FDA approved the biologics license application (BLA) submitted by BioNTech Manufacturing GmbH for COMIRNATY (COVID-19 Vaccine, mRNA) for active immunization to prevent COVID-19 caused by SARS-CoV-2 in individuals 16 years of age and older.” The efficacy claims are based on outdated data. The press release indicates that the basis of the efficacy claims was as quoted below. However, those data are outdated, and captured with strains of virus (Alpha, Beta) that are no longer predominant. The efficacy claims are therefore invalid – it is quite clear that the vaccine is much less effective in preventing infection by the currently circulating strain (Delta)
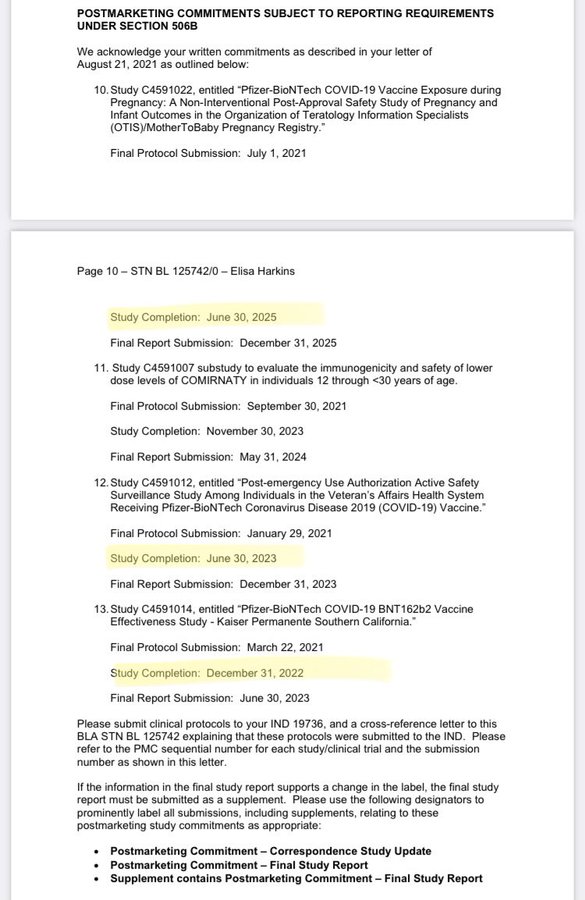
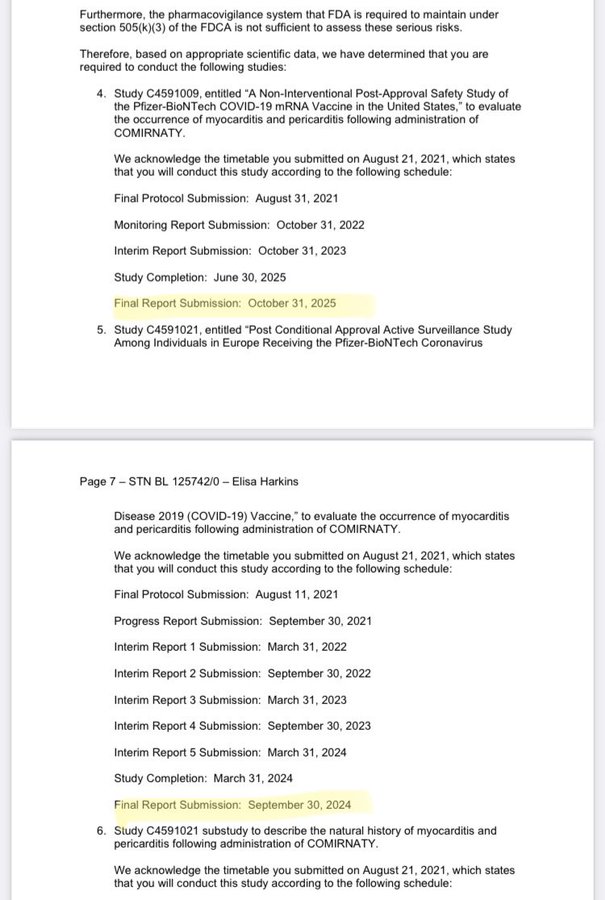
In its letter to BioNTech, the FDA states “” We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis. Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA is not sufficient to assess these serious risks.” The first sentence says that VAERS will be incapable of assessing known serious risk The second sentence says that the other pharmacovigilance systems that by law FDA employs (supposedly about 20 different databases when they were bragging about them last October) are similarly incapable of assessing known serious risk.
• The risks in pregnancy remain unknown. “although not FDA requirements, the company has committed to additional post-marketing safety studies, including conducting a pregnancy registry study to evaluate pregnancy and infant outcomes after receipt of Comirnaty during pregnancy.” The prescribing info says: “There is a pregnancy exposure registry for COMIRNATY. Encourage individuals exposed to COMIRNATY around the time of conception or during pregnancy to register by visiting https://mothertobaby.org/ongoingstudy/covid19-vaccines/ .” WHY ARE THEY DOING A PREGNANCY STUDY?
FDA has licensed the BioNTech vaccine for 16 and up
• All of the authorized vaccine on shelves and in freezers will remain only authorized, until the new product with Cominaty labelling arrives.
• 3d or booster doses and vaccine for 12-15 year olds remains under EUA
• Why not also approve the Pfizer version? Why leave it under EUA?
• When the press says the “Pfizer vaccine is fully approved.” It is not. The vaccine that is likely to be supplied for some time, WILL BE THE Pfizer – EUA vaccine. So any mandates based on full approval are meaningless.
THE BLA acknowledges LONG term myocardial issues with a 5 year follow up consistent with the lower range for LTFU for Gene Therapy Products. Is FDA quietly acknowledging the Gene Therapy classification? These products have been classified by FDA as Gene Therapy Products which require UP to 15 years long term follow up in studies. This was acknowledged by Moderna in their 2Q 2020 filing.
Using superior CDC published methods, normalizing for people vaccinated, Children’s Health Defense estimates 176x reports of VAERS deaths associated with C19 vaccines compared with flu vaccines. 35x the number for H1N1 (where stimulated reporting is speculated) Using CDC published methods we estimate under-reporting of VAERS deaths to be 5- 15x. for a total of 30,000-90,000 deaths, mostly non-C19. Underreporting for lifethreatening events may be 24-64x. IN ADDITION – (Israel MOH, combined with Dagan study), we have estimated between 35-86,000 EXCESS USA deaths due to Covid in those vaccinated (>=1 dose)
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Support the Automatic Earth in virustime. Click at the top of the sidebars to donate with Paypal and Patreon.
It’s been an insane 24 hours. You’d think a full approval of a vaccine would be a straightforward event, but the FDA just made things more, and extremely, complicated. First, a few bits and pieces from what they issued:
“COMIRNATY is the first COVID-19 vaccine to be granted FDA approval ”
also:
“These may not be all the possible side effects of the vaccine. Serious and unexpected side effects may occur. THE VACCINE IS STILL BEING STUDIED IN CLINICAL TRIALS.”
On August 23, 2021, FDA approved the biologics license application (BLA) submitted by BioNTech Manufacturing GmbH for COMIRNATY (COVID-19 Vaccine, mRNA) for active immunization to prevent COVID-19 caused by SARS-CoV-2 in individuals 16 years of age and older…
…the EUA will remain in place for the Pfizer-BioNTech COVID-19 vaccine for the previously-authorized indication and uses, and to authorize use of COMIRNATY (COVID-19 Vaccine, mRNA) under this EUA for certain uses that are not included in the approved BLA…
COMIRNATY (COVID-19 Vaccine, mRNA) is the same formulation as the PfizerBioNTech COVID-19 Vaccine and can be used interchangeably with the Pfizer-BioNTech COVID-19 Vaccine to provide the COVID-19 vaccination series…
C. There is no adequate, approved, and available [see Note 9] alternative to the emergency use of Pfizer-BioNTech COVID 19 Vaccine to prevent COVID-19.
[Note 9:] Although COMIRNATY (COVID-19 Vaccine, mRNA) is approved to prevent COVID-19 in individuals 16 years of age and older, there is not sufficient approved vaccine available for distribution to this population in its entirety at the time of reissuance of this EUA. Additionally, there are no products that are approved to prevent COVID-19 in individuals age 12 through 15, or that are approved to provide an additional dose to the immunocompromised population described in this EUA.
Conditions Related to Printed Matter, Advertising, and Promotion
X. All descriptive printed matter, advertising, and promotional material, relating to the use of the Pfizer-BioNTech COVID 19 Vaccine shall be consistent with the authorized labeling, as well as the terms set forth in this EUA, and meet the requirements set forth in section 502(a) and (n) of the FD&C Act and FDA implementing regulations.
Y. All descriptive printed matter, advertising, and promotional material relating to the use of the Pfizer-BioNTech COVID 19 Vaccine clearly and conspicuously shall state that:
” This product has not been approved or licensed by FDA, but has been authorized for emergency use by FDA, under an EUA to prevent Coronavirus Disease 2019 (COVID-19) for use in individuals 12 years of age and older; and
” The emergency use of this product is only authorized for the duration of the declaration that circumstances exist justifying the authorization of emergency use of the medical product under Section 564(b)(1) of the FD&C Act unless the declaration is terminated or authorization revoked sooner.
The original documents. Just check the dates. What happened to those?
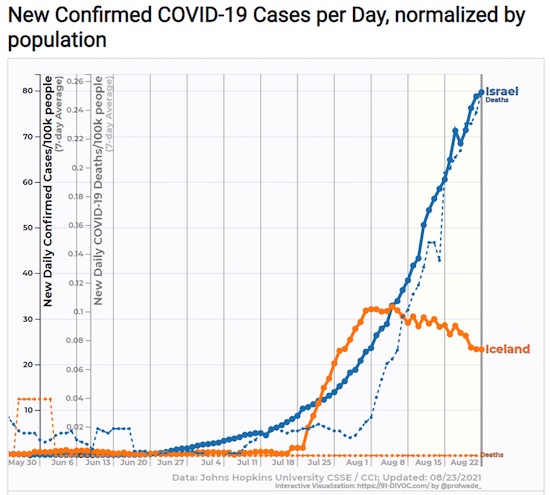
Two high vaccination rates: Iceland Full Vaxxed 74%, Israel 62%
“The Pfizer-BioNTech emergency use authorization was based on clinical trials involving about 37,000 people.”
Well, not really, because they stopped those trials.
Eight months after authorizing the Pfizer-BioNTech COVID-19 vaccine for emergency use in the USA, the Food and Drug Administration issued its full stamp of approval. Now that the companies’ detailed, so-called biologics license application has been granted, it’s likely that vaccination will be required by many companies, schools and other entities. The FDA decision clears the way for the companies to market their vaccine, which is not permitted without full licensure. And it may launch a race for booster shots, allowing doctors to prescribe extra Pfizer-BioNTech shots “off label” to anyone they think should get one. The FDA confirmed late last year through a more streamlined evaluation process that the vaccine, from pharmaceutical giant Pfizer and its partner, German startup BioNTech, was safe, effective and could be reliably produced.
The review of the 340,000-page license application was completed in just 97 days by FDA staff working “night and day,” said Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, which approves vaccines “We completed this in about 40% of the normal clock time for a submission of this magnitude,” he said. The license application was three times the size of the emergency use authorization submission, which weighed in at 110,000 pages. The companies have manufactured more than 2 billion doses, more than 200 million of which were administered in the USA, the most of any of the three vaccines allowed for use in the country. The full license includes four more months of efficacy and safety data, confirming trial results and detailing manufacturing processes.
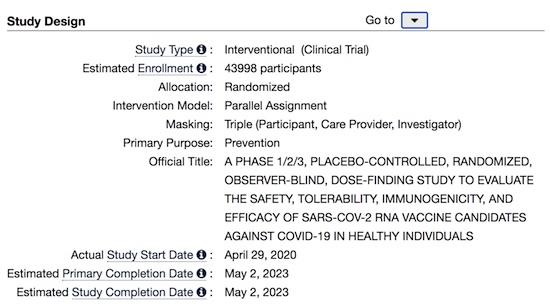
The Pfizer-BioNTech emergency use authorization was based on clinical trials involving about 37,000 people. The full approval was based on study results involving more than 44,000 people followed for six months. The license applies only to those 16 and over, but the vaccine is allowed for those 12 to 15 under the previous authorization. “Based on the longer-term follow-up data that we submitted, today’s approval for those aged 16 and over affirms the efficacy and safety profile of our vaccine at a time when it is urgently needed,” Pfizer chairman and CEO Albert Bourla said in a statement. “I am hopeful this approval will help increase confidence in our vaccine, as vaccination remains the best tool we have to help protect lives and achieve herd immunity.”
Not sure it’s a great idea for the FDA to have pissed off Peter Doshi, senior editor at The BMJ, one of the most reputable magazines around. Much more at the original (link).
On 28 July 2021, Pfizer and BioNTech posted updated results for their ongoing phase 3 covid-19 vaccine trial. The preprint came almost a year to the day after the historical trial commenced, and nearly four months since the companies announced vaccine efficacy estimates “up to six months.” But you won’t find 10 month follow-up data here. While the preprint is new, the results it contains aren’t particularly up to date. In fact, the paper is based on the same data cut-off date (13 March 2021) as the 1 April press release, and its topline efficacy result is identical: 91.3% (95% CI 89.0 to 93.2) vaccine efficacy against symptomatic covid-19 through “up to six months of follow-up.” The 20 page preprint matters because it represents the most detailed public account of the pivotal trial data Pfizer submitted in pursuit of the world’s first “full approval” of a coronavirus vaccine from the Food and Drug Administration. It deserves careful scrutiny.
[..] The elephant named “waning immunity”…“Waning immunity” is a known problem for influenza vaccines, with some studies showing near zero effectiveness after just three months, meaning a vaccine taken early may ultimately provide no protection by the time “flu season” arrives some months later. If vaccine efficacy wanes over time, the crucial question becomes what level of effectiveness will the vaccine provide when a person is actually exposed to the virus? Unlike covid vaccines, influenza vaccine performance has always been judged over a full season, not a couple months. And so the recent reports from Israel’s Ministry of Health caught my eye. In early July, they reported that efficacy against infection and symptomatic disease “fell to 64%.” By late July it had fallen to 39% where Delta is the dominant strain. This is very low. For context, the FDA’s expectation is of “at least 50%” efficacy for any approvable vaccine.
Delta may not be responsible Enter Pfizer’s preprint. As an RCT reporting “up to six months of follow-up,” it is notable that evidence of waning immunity was already visible in the data by the 13 March 2021 data cut-off… And it’s hard to imagine how the Delta variant could play a real role here, for 77% of trial participants were from the United States, where Delta was not established until months after data cut-off. Waning efficacy has the potential to be far more than a minor inconvenience; it can dramatically change the risk-benefit calculus.
The “six month” preprint based on the 7% of trial participants who remained blinded at six months Despite the reference to “six month safety and efficacy” in the preprint’s title, the paper only reports on vaccine efficacy “up to six months,” but not from six months. This is not semantics, as it turns out only 7% of trial participants actually reached six months of blinded follow-up (“8% of BNT162b2 recipients and 6% of placebo recipients had ≥6 months follow-up post-dose 2.”) So despite this preprint appearing a year after the trial began, it provides no data on vaccine efficacy past six months, which is the period Israel says vaccine efficacy has dropped to 39%. It is hard to imagine that the <10% of trial participants who remained blinded at six months (which presumably further dwindled after 13 March 2021) could constitute a reliable or valid sample to produce further findings.
Severe disease And on preventing death from covid-19, there are too few data to draw conclusions—a total of three covid-19 related deaths (one on vaccine, two on placebo). There were 29 total deaths during blinded follow-up (15 in the vaccine arm; 14 in placebo). The crucial question, however, is whether the waning efficacy seen in the primary endpoint data also applies to the vaccine’s efficacy against severe disease. Unfortunately, Pfizer’s new preprint does not report the results in a way that allows for evaluating this question.
Approval imminent without data transparency, or even an advisory committee meeting? …But here we are, with FDA reportedly on the verge of granting a marketing license 13 months into the still ongoing, two year pivotal trial, with no reported data past 13 March 2021, unclear efficacy after six months due to unblinding, evidence of waning protection irrespective of the Delta variant, and limited reporting of safety data. (The preprint reports “decreased appetite, lethargy, asthenia, malaise, night sweats, and hyperhidrosis were new adverse events attributable to BNT162b2 not previously identified in earlier reports,” but provides no data tables showing the frequency of these, or other, adverse events.) It’s not helping matters that FDA now says it won’t convene its advisory committee to discuss the data ahead of approving Pfizer’s vaccine. (Last August, to address vaccine hesitancy, the agency had “committed to use an advisory committee composed of independent experts to ensure deliberations about authorization or licensure are transparent for the public.”)
“..the jab allows vaccinated individuals to carry unusually high viral loads without becoming ill at first, potentially transforming them into presymptomatic superspreaders.”
A groundbreaking preprint paper by the prestigious Oxford University Clinical Research Group, published Aug. 10 in The Lancet, includes alarming findings devastating to the COVID vaccine rollout. The study found vaccinated individuals carry 251 times the load of COVID-19 viruses in their nostrils compared to the unvaccinated. While moderating the symptoms of infection, the jab allows vaccinated individuals to carry unusually high viral loads without becoming ill at first, potentially transforming them into presymptomatic superspreaders. This phenomenon may be the source of the shocking post-vaccination surges in heavily vaccinated populations globally. The paper’s authors, Chau et al, demonstrated widespread vaccine failure and transmission under tightly controlled circumstances in a hospital lockdown in Ho Chi Minh City, Viet Nam.
The scientists studied healthcare workers who were unable to leave the hospital for two weeks. The data showed that fully vaccinated workers — about two months after injection with the Oxford/AstraZeneca COVID-19 vaccine (AZD1222) — acquired, carried and presumably transmitted the Delta variant to their vaccinated colleagues. They almost certainly also passed the Delta infection to susceptible unvaccinated people, including their patients. Sequencing of strains confirmed the workers transmitted SARS-CoV-2 to one another. = This is consistent with the observations in the U.S. from Farinholt and colleagues, and congruent with comments by the director of the Centers for Disease Control and Prevention conceding COVID-19 vaccines have failed to stop transmission of SARS-CoV-2.
On Feb. 11, the World Health Organization indicated the AZD1222 vaccine efficacy of 63.09% against the development of symptomatic SARS-CoV-2 infection. The conclusions of the Chau paper support the warnings by leading medical experts that the partial, non-sterilizing immunity from the three notoriously “leaky” COVID-19 vaccines allow carriage of 251 times the viral load of SARS-CoV-2 as compared to samples from the pre-vaccination era in 2020. Thus, we have a key piece to the puzzle explaining why the Delta outbreak is so formidable — fully vaccinated are participating as COVID-19 patients and acting as powerful Typhoid Mary-style super-spreaders of the infection.
Vaccinated individuals are blasting out concentrated viral explosions into their communities and fueling new COVID surges. Vaccinated healthcare workers are almost certainly infecting their coworkers and patients, causing horrendous collateral damage. Continued vaccination will only make this problem worse, particularly among frontline doctors and nurses workers who are caring for vulnerable patients. Health systems should drop vaccine mandates immediately, take stock of COVID-19 recovered workers who are robustly immune to Delta and consider the ramifications of their current vaccinated healthcare workers as potential threats to high risk patients and coworkers.
So the FDA has “fully approved” the Pfizer jab for Covid. In doing so standing alone they have broken the law and thus have irrevocably destroyed their authority and any reason for anyone to ever do anything based on them ever again. Let me explain. Under black letter law an EUA is illegal if there is an alternative that is considered safe, effective and available. This was the reason the FDA did not (for 18 months!) run the studies and evaluate them on other early-intervention drugs for Covid-19. We all know what they are. I’m living proof they work too, as are millions of others worldwide. But, more-importantly, this “full approval” voids all other vaccine EUAs for Covid-19. That is, under the law the Moderna and J&J instantly became illegal to offer or use within the United States.
The makers can apply for full authorization, of course, but the EUAs are void as of this morning and under black letter law cannot be administered to anyone in the United States as they are now unlicensed and unlawful products in human beings until and unless they are given full approval themselves. No medical provider can offer or administer any other than the Pfizer Covid-19 shot in the United States as of the moment of that approval. You can bet the law will be ignored; note MRNAs stock price this morning. It should have instantly been cut in half. In addition the FDA broke the law itself when it issued the “approval.” The law requires a full hearing and the data from the full set of trials; the trials are not capable of being completed until early 2022 by the original submissions and they deliberately did not hold the hearing. This is a black letter violation of the law as well, but nobody cares.
As for me, I don’t give a crap. I’ve been infected, 98% certain it was Delta (because that’s all that’s circulating right now in the US where the index case I got infected by came from, and I know who it was) and am recovered. I hit it with meds immediately and I’m fine. I know, scientifically, it was Covid-19 and not some other virus as I now have IgG antibodies and did not for the previous 18 months which I know factually as I repeatedly tested myself. There is thus exactly zero medical benefit I can derive from the jabs. I will walk without fear into a Covid-19 ICU unit right now without any PPE on whatsoever.
I have no fear of this virus because as with every other viral infection of note including those that are much more-dangerous than Covid, such as measles, prior infection and recovery produces durable and stable immunity in essentially everyone who has a competent immune system, and I do. Those of you who trust the jabs to be equally effective to an active infection and recovery are free to come with me. I will bet my life that I’m sterile immune to the virus as a result of said infection and recovery. Are you willing to place the same bet, given the many known failures to protect by the shot, including Jesse Jackson and his wife, both of whom are in the hospital with Covid-19 despite being vaccinated in a very public spectacle in January of this year? There you have it.
According to the New York Times and multiple media outlets, Pfizer is expected to get full FDA approval today. “The move would make it the first Covid vaccine to go from emergency use authorization to full FDA approval.” With that in mind, it is worth a reminder that both Pfizer and Moderna stopped the clinical trials the FDA was using in their review: The Moderna and Pfizer vaccine tests were conducted, as customary, with a control group; a group within the trial who were given a placebo and not the test vaccine. However, during the trial -and after the untested vaccines were given emergency use authorization- the vaccine companies conducting the trial decided to break protocol and notify the control group they were not vaccinated. Almost all the control group were then given the vaccine.
Purposefully dissolving the placebo group violates the scientific purpose to test whether the vaccine has any efficacy; any actual benefit and/or safety issues. Without a control group there is nothing to compare the vaccinated group against. According to NPR, the doctors lost the control group in the Johnson County Clinicial Trial (Lexena, Kansas) on purpose: “(Via NPR) […] “Dr. Carlos Fierro, who runs the study there, says every participant was called back after the Food and Drug Administration authorized the vaccine. “During that visit we discussed the options, which included staying in the study without the vaccine,” he says, “and amazingly there were people — a couple of people — who chose that.” He suspects those individuals got spooked by rumors about the vaccine. But everybody else who had the placebo shot went ahead and got the actual vaccine. So now Fierro has essentially no comparison group left for the ongoing study. “It’s a loss from a scientific standpoint, but given the circumstances I think it’s the right thing to do,” he says.
People signing up for these studies were not promised special treatment, but once the FDA authorized the vaccines, their developers decided to offer the shots. Just so we are clear, the final FDA authorization and approval for the vaccines are based on the outcome of these trials. As noted in the example above, the control group was intentionally lost under the auspices of “the right thing to do”, so there is no way for the efficacy, effectiveness or safety of the vaccine itself to be measured. There’s no one left within the control group, of a statistically valid value, to give an adequate comparison of outcomes for vaxxed -vs- non-vaxxed. This is nuts. That NPR article is one to bookmark when people start claiming the vaccination is effective. How can the vaccine not be considered effective when there is no group of non-vaccinated people to compare the results to?
Good grief, the entire healthcare system is operating on a massive hive mindset where science, and the scientific method, is thrown out the window in favor of ideological outcomes and self-fulfilling prophecies. The fact that the researchers and doctors, apparently under the payroll of the pharmaceutical companies that have a vested financial interest in the vaccine outcome, lost the control group on purpose is alarming. Of course, Big Pharma will promote the vaccine as beneficial, and the controlled media will promote that message with a complete disconnect from the clinical trial details, and the FDA will grant approval on results that were intentionally constructed to produce only one outcome.
In Canada, informed consent to medical interventions – including vaccines – is the law. The same is true in the US, UK, EU, Australia, and New Zealand. But these governments, along with corrupt drug regulators, are now running roughshod over what were once sacrosanct laws prohibiting misleading and coercive medical procedures, and instead have unleashed a multibillion dollar media campaign of fear and mass-panic designed to pave-over the right to informed consent.
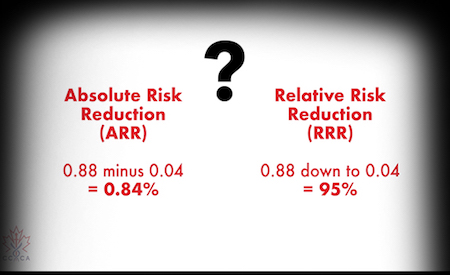
There are several systems for reporting vaccine reactions, including deaths, but the only one available to the public is VAERS. It is incomplete, because it relies on voluntary reporting, there is no incentive to report to VAERS, and it is a cumbersome process. We may compare reports of the COVID vaccines to past years, when there were also hundreds of millions of vaccinations, including annual flu shots and childhood vaccine schedules. The comparison is dramatic. There were more than twice as many deaths related to the COVID vaccines this year as the sum total of all vaccine deaths in the 30-year history of VAERS. Given this safety record, how is there any possibility of approval? Here is where the statistical fraud comes in. [I am grateful to have been alerted to this situation by Matthew Crawford]
The safety criterion they have chosen is an obscure computation called PRR for Proportional Reporting Ratio. As the name implies, it is based on RATIOS of different event types and is utterly blind to the ABSOLUTE RATE of such events. PRR measures the distribution of different kinds of adverse events, e.g. blood clots, heart attacks, and deaths. If those ratios are severely out of line with the great variety of vaccine reactions in the past, PRR would detect that. For example, if the new vaccines caused an extraordinary risk of myocarditis, but everything else was low, then PRR would flag that. But if myocarditis was just one risk among many that have been reported from past vaccines, then PRR would not pick that up.
The real scandal is that PRR is blind to the absolute risk numbers. PRR is defined in such a way as to look for unusual PATTERNS of adverse events, but it is completely insensitive to unusual RATES of adverse events. Of course, it is the rates and not the patterns that are of primary concern, and the PRR is designed NOT to reflect that.
For example, suppose we have 2 vaccines:
Vaccine A has 1 reported death per million vaccinations, 3 reported heart attacks per million, and 20 reported headaches per million.
Vaccine B has 1 reported death per hundred vaccinations, 3 reported heart attacks per hundred, and 20 reported headaches per hundred.
Vaccine A is quite safe, and vaccine B is extremely dangerous. And yet the formula for PRR will produce the same result for vaccine A and B!
Clearly, PRR is not an appropriate criterion for evaluating safety of any particular vaccine. Someone has arranged to cook the books.
“Regardless of the anti-science, despicable pieces regularly appearing in those outlets, such as suggesting that actually, masking kids is good for their learning ability.”
The push for masking, as always, boils down to a combination of incompetence, cowardice, fear, and political pressure. Experts enjoy the ability to be seen as “doing something,” and must never appear to be “anti-mask,” since it would immediately discredit them in the eyes of their peers, the greater scientific community and their ideological compatriots. Politicians want the “get out of jail free” card that masking provides; the opportunity to blame others for poor results. The “it would have worked if you’d all just listened to me” line of defense. The media simply outsources all critical thinking to like-minded ideologues and refuses to acknowledge or take seriously the few brave experts willing to tell the truth.
And as a result, corporations, whose decision makers are exclusively influenced by the same media sources, like The New York Times, follow right along. Regardless of the anti-science, despicable pieces regularly appearing in those outlets, such as suggesting that actually, masking kids is good for their learning ability. But everywhere you look, the cultural groupthink is dramatically failing. Counties and states following the CDC’s new guidance are not succeeding, and those ignoring it are faring no worse. Locations that never removed masks, such as Hawaii and Japan, are seeing their highest numbers of the pandemic, but manage to escape the vitriol and hatred leveled at Ron DeSantis because they’re following orders and implementing what the hive mind of acceptable opinion mandates.
The dramatic, predictable failure resulting from the CDC’s science-ending reversal would, in a sane world, be cause for intellectually honest experts to revisit their guidance and accept that their efforts to “control” infections is always doomed to fail. But naturally, we’re seeing the exact opposite. The more masks fail, the more we need them.
The Pentagon has said it will update its own guidance on Covid-19 vaccinations, mandating the jab for all military personnel, following the US drug regulator’s decision to fully approve the Pfizer vaccine. Speaking on Monday, US Department of Defense spokesman John Kirby said the military was aware of the Food and Drug Administration’s (FDA) decision to fully approve the Pfizer vaccine for use in people over 16, and was preparing to issue updated guidance to all service personnel. “We’re going to move forward making that vaccine mandatory,” Kirby told reporters. “We’re preparing the guidance to the force right now,” he stated, adding that the exact timetable for mandating the jab was still being worked out. Earlier on Monday, the FDA announced that the Pfizer jab had been fully approved for use in the US.
The shot has been administered under emergency-use authorization since mid-December 2020. The FDA added that the Pfizer vaccine will retain its emergency-use authorization for use in adolescents and for those requiring a third dose due to other health conditions. Earlier in August, the Washington Post reported that around 65% of active-duty military personnel were fully vaccinated, compared to around 59% of eligible Americans. Defense Secretary Lloyd Austin has previously encouraged all military personnel to get vaccinated against Covid. “To defend this nation, we need a healthy and ready force. I strongly encourage all DoD military and civilian personnel – as well as contractor personnel – to get vaccinated now and for military service members to not wait for the mandate,” Austin stated earlier in August.
As the NYT explained, education staffers are the first group of city workers to face a full vaccine mandate. The announcement also opens the door to a broader vaccine mandate of city workers, which the mayor said Monday the city was considering. Last month, Mayor Bill de Blasio issued a mandate for city workers that allowed for those unvaccinated to submit for weekly coronavirus testing. “We know this is going to help ensure that everyone is safe,” Mr. de Blasio said during a news conference on Monday, adding that city schools had extremely low virus transmission last year. The mandate, the mayor said, will help the city “build on that success.”
While the mayor’s push is likely to prove unpopular with many rank-and-file members; the city’s teacher’s unions, and unions representing other DoE staff, have signed off on the new mandate (though they’re still negotiating about what might happen to workers who continue to refuse). UFT President Michael Mulgrew acknowledged that the city had the legal right to impose the mandate, but he told reporters details were still being hashed out. The city announced last month that any teacher who failed to comply with both the vaccination requirement, and the required weekly testing for those who didn’t get the jab, would be suspended without pay.
“While the city is asserting its legal authority to establish this mandate, there are many implementation details, including provisions for medical exceptions, that by law must be negotiated with the U.F.T. and other unions, and if necessary, resolved by arbitration,” Mr. Mulgrew said in a statement. Mayor de Blasio has insisted that even if negotiations stall, the mandate will still be implemented. Meisha Porter, the chancellor of NYC’s schools, said she expects a high level of compliance from school staff on the mandate. “I do not expect a staffing shortage,” Porter said.
Australia seems to be in the grips of COVID-induced insanity as people across the country are vigorously protesting against the lockdown measures imposed to curb the spread of the renewed bout of coronavirus outbreak. After violent ruckus witnessed on the streets of major Australian cities, including Brisbane, Sydney and Melbourne, and dogs shot dead by a rural council in New South Wales to prevent volunteers from travelling during Covid restrictions, Australian truck drivers have threatened to shut down major highways across the country as a mark of protest against Covid lockdowns. Social media websites are awash with a video of a truck driver who said in his video that truck drivers are ‘planning to shut down the country’ to ‘remove the s*** government’.
He further warned the Aussies that their demonstration could end up choking supply chains and urged them to stock up on groceries to get them through the next couple of weeks. “It’s on. The truckies are doing it. The truckies are going to shut down the country,’ the man says in the video. What that means is you need to go shopping now, get what you can for the next week or two, load your fridge, freezers,” the truck driver could be seen saying in the video.
“The same progressives who regularly denounce “systemic racism” and “Western imperialism” are now enforcing policies that disproportionately punish minorities and the poor..”
Throughout the pandemic, American political and public-health leaders have been following Rahm Emanuel’s classic dictum for power-seeking officials: “You never want a serious crisis to go to waste.” Now they’ve adopted a corollary: you never want a crisis to end. So they are prolonging the national misery instead of easing it, which could be done with a few simple strategies. Explain to the public that the virus will never disappear but is no longer a mortal threat to the vast majority of Americans. Encourage the minority still at risk to get vaccinated by honestly discussing who is in jeopardy and what scientists have learned about infections. Promote treatments proven to prevent infection and speed recovery while avoiding unproven treatments and mandates that cause collateral damage and generate mistrust.
Above all, make it clear to Americans that we finally have reason to celebrate: what once seemed an unprecedented danger is now just one of many pathogens that we know how to live with. But the nation’s crisismongers aren’t about to relinquish their hold over the public, so they’ve set new goals that are as unachievable as they are unnecessary and harmful. Making vaccines available to every American adult is no longer sufficient; now the crisis cannot end until the entire population has been vaccinated. Instead of focusing efforts on vaccinating the vulnerable, officials obsess on compelling universal obedience, even if that means squandering vaccines on people who already have acquired natural immunity or are at minimal risk of serious illness.
The same progressives who regularly denounce “systemic racism” and “Western imperialism” are now enforcing policies that disproportionately punish minorities and the poor, both in the United States (the majority of black teenagers and young adults in New York have been banished from much of public life by the city’s new vaccine-passport policy) and in the rest of the world. The hypocrisy was deftly captured in a tweet by Martin Kulldorff, the Harvard epidemiologist: “If you favor university vaccine mandates for low-risk American and European students, when there is not enough vaccine for older high-risk people in Asia, Africa and Latin America, please remove your #BLM tags from your Twitter/Facebook profiles.”
Children are being sentenced to another round of unnecessary mask mandates and probably more school closures based on evidence-free warnings from Anthony Fauci and others that the Delta variant will be more deadly to them than the original virus. While the variant is more infectious, the evidence does not show it to be any more lethal. In fact, the current mortality rate among American children with Covid is lower than it was last year—and last year many more children died of the flu than of Covid. One of the most thorough studies, in England, shows that the survival rate for those under 18 with Covid is 99.995 percent. But instead of emphasizing these reassuring statistics, public-health officials like Jerome Adams, the surgeon general, keep looking for new ways to scare parents and children.
“I’m an anesthesiologist,” he tweeted last weekend. “And a dad. And I can assure you in both capacities that your child will be far more comfortable if they’re in a face mask, than on a ventilator. If you’re making a choice on behalf of a child, please choose based on their comfort, vs yours.” He offered no new evidence that children are at heightened risk from the virus, much less any evidence that a mask would make any difference, but he did make sure to include a gruesome photograph of a child on a ventilator. It was a new low in public-health demagoguery, but unfortunately not so different from the fearmongering of other officials, the press, and social-media platforms. They lament that a minority of the public remains reluctant to get vaccinated without recognizing that their own tactics are a likely a chief cause of this reluctance. They have been misleading people for so long—and censoring challenges to their misinformation—that it’s no wonder polls show that an overwhelming majority of unvaccinated Americans say they don’t trust Fauci or the CDC.
“Britain and France managed to get their nationals out last week, only to be rebuked by American brass for “making us look bad.” That helped, I’m sure.”
Notice, there are two sets of hostages in this phase of what looks like an engineered US collapse: the thousands of stranded Americans who can’t get out of Afghanistan thanks to the history-rockin’ ineptitude of “Joe Biden,” Tony Blinken, and General Mark Milley, and the millions of We-the-People back home whose minds are hostage to the narratives concocted in a shadowland of sinister governance. Welcome to a week of throwdowns and showdowns, a force majeure of mind change. A strange paralysis in the Pentagon has prevented the use of US power to clear an escape corridor to Kabul’s airport and establish order in the facility — this, after the tactically mystifying decision to abandon the US Bagram military airfield, a good twenty miles outside of festering Kabul, and surrounded by more easily-securable empty desert.
Britain and France managed to get their nationals out last week, only to be rebuked by American brass for “making us look bad.” That helped, I’m sure. And then how long can the stranded Americans even stay hidden and alive? They have to eat. Either they come out of their hidey-holes and get to some market, or they would (theoretically) have to send some Afghani servants to fetch them supplies, But, what Afghani in his right mind would want to be caught in service to the Americans by the Taliban? That quandary must have a pretty short time-horizon on it. Standing by to see how it works out….
Next in this week’s throwdown parade is the FDA’s imminent approval of Pfizer’s Covid-19 vaccine, without any of the usual extensive trials. How does that even happen, with an efficacy rate of 39 percent maximum and a runaway train of vicious side effects ranging from brain and heart damage to infertility? The so-called mRNA “vaccines” are also implicated in the ongoing mutation of the disease, producing a cavalcade of variants. Is that, perhaps, on-purpose, to keep the pandemic going, preventing it from burning-out?
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Consent
Excellent points by Canadian criminal defence lawyer, Nicholas Wansbutter, arguing vaccine passports would be anti-consent, and that the case law makes clear it is an assault.https://t.co/NUmAx8VPIdpic.twitter.com/0gWbzLuC46
The FDA will give full authorization to Pfizer’s Covid jab sometime next week, according to multiple reports, putting it on track to be the first in the US to get approval and likely paving the way for additional vaccine mandates. The US regulator is expected to give the greenlight for Pfizer’s immunization in the coming days, the New York Times and Politico reported on Friday, citing several “people familiar” with the agency’s planning. Though the FDA still has a “substantial amount of paperwork and negotiation with the company” to get through, it could give full approval as soon as Monday, the Times added. It was previously reported that the FDA hoped to grant authorization before Labor Day on September 6, and now appears set to meet that informal deadline.
With a number of hospital systems and universities around the US signaling plans to mandate vaccinations against Covid-19 upon full approval, the move is likely to trigger a spate of new requirements around the country. The US military, moreover, has also said it would compel immunizations for its 1.3 million active-duty troops by the middle of next month, but could do so sooner should the FDA give its blessing to Pfizer. While the Joe Biden administration previously suggested the president would issue a waiver to allow vaccine mandates for soldiers, it decided to hold off until regulators signed off.
Reports of the FDA’s plans come soon after the White House began promoting booster shots for all fully vaccinated adults, citing US health agencies, which noted the immunizations are losing effectiveness over time, particularly against more infectious Delta mutation. While the FDA hasn’t yet approved third doses for all healthy Americans, the agency did give the go-ahead for those with compromised immune systems, while Pfizer recently submitted its initial trial data for universal boosters. Health officials have voiced hopes that full approval for the Covid jabs could improve vaccination numbers in the US, which have been losing pace since hitting a peak in April. Recent polling by the Kaiser Family Foundation showed that more than 30% of respondents would be “more likely” to be vaccinated if the FDA authorized the shots, suggesting the move could indeed spur immunizations.
On August 5 (last update), this was still up on clinicaltrials.gov for the Pfizer trials:
Transparency advocates have criticised the US Food and Drug Administration’s (FDA) decision not to hold a formal advisory committee meeting to discuss Pfizer’s application for full approval of its covid-19 vaccine. Last year the FDA said it was “committed to use an advisory committee composed of independent experts to ensure deliberations about authorisation or licensure are transparent for the public.”1 But in a statement, the FDA told The BMJ that it did not believe a meeting was necessary ahead of the expected granting of full approval. “The FDA has held numerous meetings of its Vaccines and Related Biological Products Advisory Committee (VRBPAC) related to covid-19 vaccines, including a 22 October 2020 meeting to discuss, in general, the development, authorisation, and licensure of covid-19 vaccines,” an FDA spokesperson said.
“The FDA also has held meetings of the VRBPAC on all three covid-19 vaccines authorised for emergency use and does not believe a meeting is needed related to this biologics license application.” The spokesperson added, “The Pfizer BioNTech covid-19 vaccine was discussed at the VRBPAC meeting on 10 December 2020.3 If the agency had any questions or concerns that required input from the advisory committee members we would have scheduled a meeting to discuss.” The vaccine has already been rolled out to millions of Americans through an emergency use authorisation. Companies typically apply for full approval after a longer period has elapsed so that more data are available for review.
But with the US government indicating this week that it plans to start making booster shots widely available next month, experts said the decision not to meet to discuss the data was politically driven. Kim Witczak, a drug safety advocate who serves as a consumer representative on the FDA’s Psychopharmacologic Drugs Advisory Committee,4 said the decision removed an important mechanism for scrutinising the data. “These public meetings are imperative in building trust and confidence especially when the vaccines came to market at lightning speed under emergency use authorisation,” she said. “The public deserves a transparent process, especially as the call for boosters and mandates are rapidly increasing. These meetings offer a platform where questions can be raised, problems tackled, and data scrutinised in advance of an approval.”
Witczak is one of the more than 30 signatories of a citizen petition5 calling on the FDA to refrain from fully approving any covid-19 vaccine this year to gather more data. She warned that without a meeting “we have no idea what the data looks like.” “It is already concerning that full approval is being based on 6 months’ worth of data despite the clinical trials designed for two years,” she said. “There is no control group after Pfizer offered the product to placebo participants before the trials were completed. “Full approval of covid-19 vaccines must be done in an open public forum for all to see. It could set a precedent of lowered standards for future vaccine approvals.”
In the 1960s, scientists found that antiviral antisera might result in an exceptional increase in viral infectivity of animal viruses. This phenomenon that viral infection can be enhanced by internalization associated with antibody Fc receptors (FcRs), denoted as ‘antibody-dependent enhancement’ (ADE; Box 1), was then widely reported in infections with flaviviruses and other viruses. Later, more antibody FcR-mediated effects, such as complement activation and release of inflammatory cytokines, were reported to be involved in severer disease. ADE has also been observed in vaccinated animals after viral challenge with the corresponding virus.
For example, cats immunized with a vaccine expressing the feline infectious peritonitis virus (FIPV) S protein on a recombinant pox virus vector died earlier than control animals when challenged with FIPV25. Given that passive immunization with feline serum containing high-titre antibodies reactive with feline FIPV also resulted in a more rapid disease after FIPV challenge, the vaccine-induced disease exacerbation may be attributed to ADE. Apart from ADE, type 2 T helper cell (TH2 cell)-based immunopathologic responses induced by homologous viral challenge after vaccination could also result in disease exacerbation.
In this Perspective, we use the term ‘vaccine-associated disease enhancement’ (VADE; Box 1) to describe both antibody-dependent and TH2 cell-dependent disease exacerbation (Fig. 1). We summarize examples of VADE in the history of the development of vaccines against respiratory syncytial virus (RSV), dengue virus (DENV), SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV), each of which provides clues for safe COVID-19 vaccine development and highlights the need for rigorous preclinical and clinical safety testing.
There have been warnings that ADE should be fully evaluated for coronavirus vaccines to avoid repeating the tragic failure of the RSV vaccine. The first RSV vaccine, based on formalin-inactivated RSV (FI-RSV), entered a clinical trial in 1965, a time when several other inactivated or attenuated virus-based vaccines had already been successfully developed, such as vaccines against smallpox and polio. The FI-RSV vaccine was well tolerated and appeared to be moderately immunogenic at first. However, instead of protecting study participants, the FI-RSV vaccine exhibited a paradoxical disease-strengthening effect (enhanced respiratory disease (ERD); Box 1) during subsequent natural RSV infection. Among the 20 infants who received the FI-RSV vaccine, 16 required hospitalization, including two who subsequently died, whereas only one of the 21 participants in the control group was hospitalized. The FDA then urgently suspended all clinical studies of RSV vaccines.
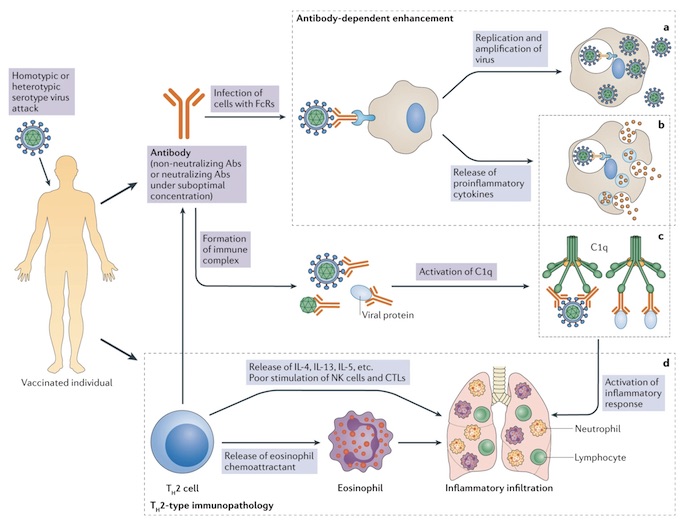
Vaccination induces humoral and cellular immune response in immunized individuals. In the normal condition, when the homologous virus enters an immunized body, it will be neutralized or cleared by vaccine-induced neutralizing antibodies (Abs) or specific T cells, respectively. In the context of vaccine-associated disease enhancement, vaccines mainly induce non-neutralizing Abs or low titres of neutralizing Abs (suboptimal concentration) or type 2 T helper cell (TH2 cell)-biased T cell responses. When these vaccinated individuals are challenged by homotypic or heterotypic serotype viruses, the antibodies will immediately recognize the viruses and mediate antibody-dependent disease exacerbation in two ways. First, virus–antibody complexes might enter Fc receptor (FcR)-bearing cells, such as dendritic cells and monocytes, by FcR-mediated internalization, which is termed ‘antibody-dependent enhancement’ (ADE). For viruses with innate tropism for FcR-bearing cells, such as dengue virus, ADE will result in higher viral loads than in conditions without antibodies.
a | After entry, the virus, no matter whether it replicates or does not replicate, may activate a harmful immune response, resulting in the release of proinflammatory cytokines. b | Aside from ADE, antibody–antigen complexes can stimulate the complement pathway through activation of the C1q pathway, thus further strengthening the inflammatory responses c | Vaccine-associated disease enhancement can also involve a TH2 cell-biased immune response. The activated TH2 cells contribute to the activation of antibody production. However, they release interleukin-4 (IL-4), IL-13 and IL-5, as well as eosinophil chemoattractant, thus resulting in eosinophil infiltration and proinflammatory cytokine production in the lung. d | Natural killer (NK) cells and CD8+ cytotoxic T lymphocytes (CTLs) are poorly stimulated in TH2 cell-skewed immune responses. The exaggerated cytokine release (part b), activation of the complement pathway (part c) and the excessive mobilization of eosinophils all contribute to the infiltration of the lung by eosinophils, neutrophils and lymphocytes, and production of inflammatory cytokines (part d), leading to acute lung injury or acute respiratory distress syndrome.
Blame unvaccinated people, blame Florida all you want. The vaccine still didn’t work. How do you not reach that conclusion?
And his doctor is a doofus who says there’s a “one-in-a-million” chance of a “breaktrough” infection. He should get informed. There’s an every hour, if not more.
A fully vaccinated man who resided in a Florida retirement home died from COVID-19. His daughters wrote an obituary urging people to get vaccinated and blame the state for his life ending. Clark Allen died on July 22 after contracting a breakthrough case of COVID-19, a “one-in-a-million” chance, according to the man’s doctor. The surviving daughters of Clark Allen, Danielle and Nicole Allen-Gentile, expressed their anger in an obituary about how their father could have been infected and said his death was preventable, The Washington Post reported. America is changing faster than ever! Add Changing America to your Facebook or Twitter feed to stay on top of the news.
“He was infected by someone who chose to not get vaccinated and his death was preventable,” the obituary reads. “It is the wish of his family that everyone get vaccinated in order to prevent further death, sickness and heartbreak.” The daughters also told The Washington Post that if their father were in a different state, they believe he wouldn’t have died. During the pandemic, Clark Allen’s two daughters — along with their five siblings — debated whether their father should be in an assisted living home in Florida or Connecticut. The daughters received a blunt message from a Connecticut home: “You need to get him out of Florida. He will die in Florida,” The Washington Post reports. The daughters speculate that he contracted the virus from an unvaccinated person at Carlisle Palm Beach, an assisted living facility in Lantana, Fla.
Allen reportedly took the virus very seriously, paying close attention to public health measures as he had chronic obstructive pulmonary disease that could make a possible infection more severe, according to the Tampa Bay Times, which first shared the story. “It was a relief when he got vaccinated, but the reality was he was around a lot of unvaccinated people,” Danielle Allen, who lives in Portland, Ore., told The Post. “I’m attempting to not be very angry at unvaccinated people and it’s become extremely difficult. We’re all really angry and struggling.” In response to the claim, a spokesperson for Senior Lifestyle, the company that operates Carlisle Palm Beach, told The Post that its facility implements safety measures provided by Centers for Disease Control and Prevention (CDC) and “other expert sources and health authorities.”
“The system delivers medicine to intramuscular and subcutaneous tissue depths without needles, which may prove particularly useful in a world competing for needles and syringes.”
India’s drug regulator has approved a three-dose Covid-19 vaccine which uses plasmid DNA technology developed by indigenous drugmaker Zydus Cadila, after trials indicated it was 66.6% effective. On Friday, the Drug Controller General of India gave the green light to Zydus Cadila’s Covid-19 vaccine. The inoculation, now the sixth such to be approved in India, has received Emergency Use Authorization (EUA) for use in adults and children aged 12 and above. The generic drugmaker, which applied for authorization of its three-dose vaccine in July, enlisted 28,000 volunteers into its trial. Data from the late-stage trial suggested the jab was 66.6% effective at preventing symptomatic Covid-19.
The vaccine, known as ZyCoV-D, is the world’s first vaccine against Covid-19 that uses plasmid DNA technology. It works by injecting genetically-engineered plasmid containing the DNA sequence of the pathogen. Cadila’s vaccine was developed in partnership with India’s Department of Biotechnology and is the second home-grown shot to be approved for use against Covid-19; the first being Bharat Biotech’s Covaxin jab. Instead of traditional syringes, the vaccine is administered using a needle-free applicator. The system delivers medicine to intramuscular and subcutaneous tissue depths without needles, which may prove particularly useful in a world competing for needles and syringes.
Cadila has already started stockpiling its vaccine and hopes to make 100 million to 120 million doses every year, enough for 40 million people, the company’s managing director told Reuters in April. Despite being one of the world’s largest vaccine manufacturers, India’s Covid-19 inoculation program has fallen flat amid a shortage of shots. Delhi has been pushing for ‘Atmanirbhar Bharat’, a Hindi phrase roughly translating as ‘self-reliant India’, in a number of fields, including defense technology and medical products. The vaccination program was meant to reflect India’s self-reliance and burgeoning manufacturing capacity in the medical and pharmaceutical industry.
Ivermectin has more than one potentially effective mechanism of action against Covid 19. A major one is its ability to adhere to the Coronavirus Spike1 protein at various strategic points used by the virus to bind and enter our cells. For this reason, unlike monoclonal antibodies, it can act against all variants. By doing so, you prevent the virus from attaching itself to ACE2, which is the main gateway for the virus to enter our cells, and this allows it to reduce the virus’s ability to enter our body. If Covid stays outside of our cells, it becomes easy prey for our immune system, which can get rid of it much more easily. It is important to note that the protein docking region of the virus, the spike spikes, binds not only to our ACE2 receptors, but also to other docking receptors that are very important to the virus, those that depend on sialic acid, Receptor CD147 and on a cholinergic receptor called a7nAChr. I don’t want to get into technicalities, but this premise helps us understand how Covid attacks our body.
Once it has entered our lungs and damaged them, the virus enters the blood and travels through our body carried by red blood cells and platelets that are found in large quantities in our blood. Today we know that the virus attaches itself to red blood cells and platelets because both are coated with sialic acid receptors and CD147 and thanks to this it invades all blood vessels until it is “released” into the endothelium (the inner part of our blood vessels ). ) and then causes systemic vasculitis, which is why most of us are ultimately unable to overcome the infection. When the virus replicates within the endothelial cells of the vessels, it inflames them and creates sticky aggregates of red blood cells and platelets – dense masses,Small clots that initially hamper cause circulation in small vessels (capillaries), but then progressively swell and block larger and larger vessels. When this happens in the lungs, it causes a lack of oxygen that therefore damages all our organs such as the brain, liver, kidneys and heart, especially in the elderly, diabetics and people with previous diseases.
The mechanism by which the virus moves in the blood also explains why Covid is more lethal in people with high glucose levels, such as diabetics and prediabetics. The reason is because the receptors made of sialic acid and CD147 are basically zuccheri. In a diabetic, these sialic acids are richer in sugar (glucose) and the virus sticks better and its systemic spread is even easier. This selectivity of the virus for the characteristics of some subjects is also given by blood groups, for example those with blood group A or B have red blood cells with a greater presence of sialic acid / sugars on the surface, while those with a Type 0 blood group, on the other hand, is less susceptible to the virus as it has less sialic acid / receptor that lines red blood cells and,therefore, the virus sticks less. Patients with diabetes or those with these blood groups (A and B) have a statistically more severe course of the disease.
One of the fundamental mechanisms by which ivermectin acts in patients is because it “puts a wall” (a shield) between our body (red blood cells, platelets and vessels) and the virus, and therefore no longer allows it to latch on in our cells. thus facilitating the flow of red blood cells that carry oxygen in the blood vessels. Ivermectin appears to be able to quickly break the link between the virus (Spike’s key) and its receptors (the ACE2 gate, sialic acids, the CD147 receptor, and a7nAChr), so patients miraculously begin to breathe and oxygenate properly again normally within 24- 48 hours. This is also what happens in the rest of the microcirculation of the whole body and leads to the rapid improvement of the functionality of the various organs.
Anecdotal evidence detailed by former Google software engineer Mike Hearn strongly suggests that most restaurants, cafes and other businesses in France are not enforcing the country’s controversial vaccine passport system. As we highlighted last week, on the first day the new program was in place, police were visibly patrolling bars and cafes demanding customers show proof they’ve had the jab. However, this seems to have largely been a bluff as just days later, businesses and venues have become very lax at checking people’s papers despite the threat of large fines. “I decided to do a simple experiment to find out: always present an expired test even though I had a valid negative one, and see what happens,” writes Hearn.
“Over a four day stay I was required to show a valid pass exactly zero times; that includes at the airports in both directions. Compliance is absolutely min viable and often lower.” “At small businesses enforcement was non-existent: sometimes the pass requirement was ignored entirely, other times we were asked “do you have a pass” and our answer wasn’t checked. One restaurant had come up with a clever way to detect police stings without requiring customers to actually present a pass. As expected, enforcement was stricter by larger firms, however even there we saw the following:
– Test certificates being checked once and then swapped for a token that doesn’t expire.
– Expired tests being accepted.
– People accepting paper test certificates without scanning them.
– Scanning tests and then not looking at the screen to see the results.
– Accepting QR codes that failed to scan.”
Hearn also reveals how mask mandates in theme parks and other venues are also not being followed, despite signs everywhere ordering people to cover their faces, while social distancing is also a “forgotten memory.” Images showing empty cafes and bars on the first day the system was introduced may have spooked venues into taking a hands off approach. In passing the law but failing to ensure that it is enforced, France is following the same model as Israel, where the point of introducing the system wasn’t really to enforce it, but merely as a means of bullying young people into getting the vaccine. As we highlighted last week, despite the odious and draconian nature of the vaccine passport system, President Macron asserted that the it was actually introduced to protect people’s “freedom,” which is like saying putting you in prison is for your own safety.
Nearly 90% of people across the UK are “likely or very likely” to accept a third Covid-19 jab if offered, a new survey released by the Office for National Statistics (ONS) has revealed. On Friday, the ONS released the latest data from its ongoing Opinions and Lifestyle Survey project, which found that a whopping 87% of respondents would be in favour of receiving a Covid booster shot. Older members of the population expressed more enthusiasm at the prospect of a third jab, with almost 96% of those aged 70 or over saying they would be “likely or very likely” to do so. The survey figure was lower for younger Britons in the 16 to 29 age-bracket, standing at 78%. Speaking to reporters on Thursday, Britain’s Health Secretary Sajid Javid said that the proposed booster scheme will likely start in September. Javid, however, did not pinpoint an exact date, citing that the government first needs final advice on the matter from the Joint Committee on Vaccination and Inoculation (JCVI).
A handful of countries have already introduced a booster dose as part of their vaccination regimens. Serbia and Hungary began offering its citizens a third Covid shot earlier this month, while Israel continues to lower the eligible age for its booster jabs after rolling out the scheme at the end of July. The head of the WHO Tedros Adhanom Ghebreyesus urged nations to pause or delay issuing third shots in a bid to alleviate vaccine inequity between high and low income states. “WHO is calling for a moratorium on boosters until at least the end of September, to enable at least 10% of the population of every country to be vaccinated,” he implored the governments of richer nations. The JCVI last month recommended that all adults in the UK aged 50 and over, pensioners living in care homes, frontline workers, and anyone aged 16 and higher who is clinically vulnerable or immunocompromised should be offered a vaccine top-up this autumn.
Jimmy Carter was undone by a mere fifty-two hostages in Iran, 1979, but this fiasco is orders of magnitude greater. The Taliban could easily put an end to the whole question of extracting the thousands of Americans stuck in Af-stan just by firing a few RPG rounds onto the runway of Hamid Karzai International Airport. After that, would they go about the grisly business of beheading any Afghani who so much as took a stick of gum from an American?
“Graveyard of Empires,” indeed. Rome waited a few centuries to collapse but America seems to be demonstrating we can git’er done in just a couple of years. And, beyond these questions of global hegemony, there is the matter of what happens here in the so-called Homeland. The Covid-19 vaccine-and-masking hysteria is coming to a head. The school boards are getting an earful about race-based everything in the curriculum. Certain state governors and mayors seem determined to destroy what remains of small business. A mutiny is brewing against Bill de Blasio’s new semi-lockdown in New York City. Gavin Newsom is about to be tossed into the North Pacific Gyre.
Any moment, the Arizona election audit will issue a preliminary report, said to be shocking. Financial markets are in the wobble-zone. Supply lines are down for many parts of things needed to run daily life in this land. And millions are wondering anxiously now: what really are the latent effects of those jabs? Things are shaking loose all over the place. As Bob Dylan once said, the order is rapidly fading (and he’s even older than “Joe Biden.”) Everyone I know has got the heebie-jeebies. Nobody is at the controls of this outfit as we sail into the fog.
Mark Crispin Miller is Professor of Media, Culture and Communication at New York University. His research interests include modern propaganda, history and tactics of advertising, American film, and media ownership. He is the author of Boxed In: The Culture of TV; Seeing Through Movies; Mad Scientists: The Secret History of Modern Propaganda; Spectacle: Operation Desert Storm and the Triumph of Illusion; and The Bush Dyslexicon.
Renowned physician and professor of medicine Dr. Peter McCullough describes early treatment protocols for COVID-19 that have saved countless lives… and the forces that have aligned themselves against their widespread adoption.
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Just totally not
.@DavidMuir: "The president said he has no intelligence that the Americans have not been able to get [to the Kabul airport]. The question, obviously—does that square with reporting on ground?"@IanPannell: "I mean—just totally not."pic.twitter.com/xJhqHIaRAI
It is very important that people understand what is happening here. The intention is to introduce vaccine passports everywhere. But this is a disguise. It’s a world’s first digital common-format, globally-interoperable ID system with an editable health flag (vaccinated Y or N). It makes no one safer. If you’re vaccinated, you’re protected & are not made safer by knowing others immune status. As in Israel, you will be compelled to present a valid VaxPass in order to access defined facilities or access services. No VaxPass, you’re denied. This system only needs 50%+ of the adult population to start up because of its huge, coercive power on the unvaccinated. It’s illegal, medical apartheid. If they succeed, it won’t help you to refuse. They’ll move on, leaving that minority behind.
A VaxPass System like this will give to those controlling the database & it’s algorithms TOTALITARIAN TYRANNY over us all. The ONLY way to stop this biosecurity nightmare is to NOT GET VACCINATED FOR NON-MEDICAL REASONS!!! I fear that, if our adversaries gain this absolute control, they will use it to harm the population. There’s no limit to the evil which will flow from this strategic goal. DO NOT ALLOW THIS SYSTEM TO START UP, because it’s unstoppable afterwards. One example: your VaxPass pings, instructing you to attend for your 3rd or 4th or 5th booster or variant vaccine. If you don’t, your VaxPass will expire & you’ll become an out-person, unable to access your own life. How much choice do you have? It’s none. You are controlled. Forever. PLEASE share this widely, on every platform you use.
Pfizer and BioNTech began the process of applying for full FDA approval of their Covid-19 vaccine Friday, an expected move that could force the issue of whether vaccine mandates—proposed for schools, colleges and even some workplaces—will be a legal way to combat the virus. The Pfizer vaccine has been used in the U.S. under an emergency use authorization since December, a designation that requires companies to continue clinical trials and work towards full approval. Full approval would mean the vaccine can stay on the market once the pandemic emergency is over, important if we are to remain vigilant against circulating pockets of coronavirus and counter novel variants.
A full license adds a new dimension to the debate over whether organizations, schools and universities are allowed to require vaccination, with many opponents arguing that people cannot be required to get a vaccine licensed under an emergency use authorization. Legally speaking, there hasn’t really been a test as to whether a temporarily authorized vaccine can be mandated, Carmel Shachar, executive director of Harvard’s Petrie-Flom Center, told Forbes, though a fully licensed vaccine would certainly “be less controversial to mandate.” While any mandate would have to take account of legally protected medical and religious exemptions, Shachar said any further accommodations—such as an opposition to vaccination—would be decided by the organization implementing it and relevant local laws.
Shachar added that it “would not be that much of a stretch” to add a Covid-19 vaccine to the “long list” of vaccines children need to get in order to attend school or daycare. [..] A fully approved vaccine could have a significant impact on persistent vaccine hesitancy in the U.S.. Polls commonly record people waiting to see if the vaccines are safe as a reason for refusing a shot, something Field said often stems from a “misconception out there about the nature of an” emergency authorization. Many believe the designation means they are still “experimental,” Field said, despite ample evidence demonstrating safety and efficacy. Hesitancy appears to be particularly strong in parents, many of whom have doubts over vaccinating their children. However, experts say vaccinating children will be vital to protect them and keep the community safer.
“..during January-February 2021, at the peak of the Israeli mass vaccination campaign, there was a 22% increase in overall mortality in Israel compared with the previous year.” “In fact, January-February 2021 have been the deadliest months in the last decade..”
The Israeli People Committee (IPC), a civilian body made of leading Israeli health experts, has published its April report into the Pfizer vaccine’s side effects indicating damage to almost every system in the human body. If the findings by IPC are genuine, then Pfizer vaccine is linked to more deaths in Israel than AstraZeneca’s in the whole of Europe. The findings are catastrophic on every possible level. This is a detailed report that highlights the most devastating findings. The verdict of the Israeli People Committee is that “there has never been a vaccine that has harmed as many people.” The report is long and detailed. “We received 288 death reports in proximity to vaccination (90% up to 10 days after the vaccination), 64% of those were men.”
Yet the report states, “according to data provided by the Ministry of Health, only 45 deaths in Israel were vaccine related.” If these are the genuine numbers, then Israel has failed to report on its experimental results genuinely. We have been hearing a lot about the rare side effects of the AstraZeneca vaccine and more than 300 cases of blood clots found in Europe. German scientists have found the exact 2 step process how the AstraZeneca COVID-19 vaccine causes blood clots in recipients. They describe a series of events that has to happen in the body before the vaccines create these large clots. If the findings by IPC are genuine, then Pfizer vaccine is linked to more deaths in Israel than AstraZeneca’s in the whole of Europe.
Meanwhile, the US CDC and FDA have lifted their recommended pause on use of Johnson & Johnson’s coronavirus vaccine with a condition that it will now include a safety label warning that its vaccine comes with blood clot risks. “According to Central Bureau of Statistics data during January-February 2021, at the peak of the Israeli mass vaccination campaign, there was a 22% increase in overall mortality in Israel compared with the previous year.” “In fact, January-February 2021 have been the deadliest months in the last decade, with the highest overall mortality rates compared to corresponding months in the last 10 years.” The IPC finds that “amongst the 20-29 age group the increase in overall mortality has been most dramatic. In this age group, we detect an increase of 32% in overall mortality in comparison with previous year.”
“Statistical analysis of information from the Central Bureau of Statistics, combined with information from the Ministry of Health, leads to the conclusion that the mortality rate amongst the vaccinated is estimated at about 1: 5000 (1: 13000 at ages 20-49, 1: 6000 at ages 50-69, 1: 1600 at ages 70+).” “According to this estimate, it is possible to estimate the number of deaths in Israel in proximity of the vaccine, as of today, at about 1000-1100 people.”
The European Medicines Agency (EMA) is investigating reports of AstraZeneca’s Covid-19 vaccine causing Guillain-Barre syndrome, as the pharmaceutical company remains embroiled in controversy over the jab’s link to blood clotting. In a meeting this week, the European Medicines Agency’s Pharmacovigilance Risk Assessment Committee (PRAC) revealed that it was “assessing reports” of the rare immune system disorder being found in people following vaccination. “As part of the review of the regular pandemic summary safety reports for Vaxzevria, AstraZeneca’s Covid-19 vaccine, the PRAC is analysing data provided by the marketing authorization holder on cases of Guillain-Barre syndrome (GBS) reported following vaccination”, the PRAC declared.
“GBS was identified during the marketing authorization process as a possible adverse event requiring specific safety monitoring activities”, the committee continued, adding that it has requested “further detailed data” on the cases and will release new information as it becomes available. According to the UK’s National Health Service (NHS), Guillain-Barre syndrome is a “very rare and serious condition that affects the nerves”, and can create feelings of numbness, weakness, and pain in those who have it. Though the NHS advises that Guillain-Barre syndrome is a treatable condition and that “most people will eventually make a full recovery”, it can also be life-threatening and leave those who have had it with “long-term problems”
Following hundreds of cases of blood clotting – and dozens of deaths – AstraZeneca’s Covid-19 vaccine has already been restricted in many countries to older people only. In the UK, those under the age of 40 are set to be offered an alternative vaccine provided this causes no “delays” in the vaccination program, however the European Medicines Agency maintains that the vaccine’s benefits outweigh the risk for much of the population.
A team of prominent scientists has doubled down on its controversial hypothesis that genetic bits of the pandemic coronavirus can integrate into our chromosomes and stick around long after the infection is over. If they are right—skeptics have argued that their results are likely lab artifacts—the insertions could explain the rare finding that people can recover from COVID-19 but then test positive for SARS-CoV-2 again months later. Stem cell biologist Rudolf Jaenisch and gene regulation specialist Richard Young of the Massachusetts Institute of Technology, who led the work, triggered a Twitter storm in December 2020, when their team first presented the idea in a preprint on bioRxiv. The researchers emphasized that viral integration did not mean people who recovered from COVID-19 remain infectious.
But critics charged them with stoking unfounded fears that COVID-19 vaccines based on messenger RNA (mRNA) might somehow alter human DNA. The critics also presented a brace of scientific criticisms, some of which the team addresses in a paper released online today by the Proceedings of the National Academy of Sciences (PNAS). “We now have unambiguous evidence that coronavirus sequences can integrate into the genome,” Jaenisch says. SARS-CoV-2, the virus that causes COVID-19, has genes composed of RNA, and Jaenisch, Young, and co-authors contend that on rare occasions an enzyme in human cells may copy the viral sequences into DNA and slip them into our chromosomes. The enzyme, reverse transcriptase, is encoded by LINE-1 elements, sequences that litter 17% of the human genome and represent artifacts of ancient infections by retroviruses.
In their original preprint, the researchers presented test tube evidence that when human cells spiked with extra LINE-1 elements were infected with the coronavirus, DNA versions of SARS-CoV-2’s sequences nestled into the cells’ chromosomes. Many researchers who specialize in LINE-1 elements and other “retrotransposons” thought the data were too thin to support the claim. “If I would have had this data, I would have not submitted to any publication at that point,” says Cornell University’s Cedric Feschotte, who studies endogenous retrovirus chunks in the human genome. He and others also said they expected higher quality work coming from scientists of the caliber of Jaenisch and Young. In two subsequent studies, both posted on bioRxiv, critics presented evidence that the supposed chimeras of human and viral DNA traces are routinely created by the very technique the group used to scan for them in chromosomes.
“In January and February of 2020, hundreds of Americans in Wuhan, China, were flown back to the U.S. Considering how many people had died of COVID-19 in China at that point, it would have made sense to test those Americans who were coming back.”
“No one should have to be as brave as Charity Dean was as a local public health officer. To do her job, she had to be brave in a way that brought tears to my eyes,” Lewis tell NPR. “And when I first met her, I realized I had a character because all over her house were like these Post-it notes reminding her to be brave, like … ‘courage is a muscle memory’ or ‘the tallest oak in the forest was once just a little nut.’ She had all these kind of inspirational things. And when you get into the story of what Charity Dean … had to do on the ground, your hair stands up on the back of your neck.” Lewis writes about how Dean tried and tried to get the state officials around her to look at the data and act to make sure the virus didn’t spread. She put it all on the line, her reputation, her job.
And across the country, there was another group of doctors led by Carter Mescher trying to do the same thing at the federal level. “It was incredible to me that there was this kind of secret group of seven doctors — they called themselves the Wolverines — who were positioned in interesting places in and around the federal government, who had been together for the better part of 15 years and who had come together whenever there was a threat of a disease outbreak to help organize the country’s response,” Lewis says. But by 2020, the Trump administration had disbanded the pandemic response unit and these doctors were forced to go rogue. A mutual acquaintance put Charity Dean in touch with Carter Mescher.
“And Charity picked up all of Carter Mescher’s analysis. And she said it was like pouring water on a dying plant, that it was the first person she met who was thinking about this threat the way she was thinking about it,” Lewis says. “And so she’s very soon on the private calls. … Think of her as an actual battlefield commander. She’s in the war, in the trenches, as if she’s figured out in the course of her career in public health that there are no generals or the generals don’t understand how the, how the battle’s fought. And she’s going to have to kind of organize the strategy on the field.” In January and February of 2020, hundreds of Americans in Wuhan, China, were flown back to the U.S. Considering how many people had died of COVID-19 in China at that point, it would have made sense to test those Americans who were coming back.
But according to Lewis and his sources, then-CDC Director Robert Redfield refused to test them, saying it would amount to doing research on imprisoned persons. “Redfield is a particularly egregious example, but he’s an expression of a much bigger problem. And if you just say, ‘oh, it’s the Trump administration’ or ‘oh, it’s Robert Redfield,’ you’re missing the bigger picture,” Lewis says. “And the bigger picture is we as a society have allowed institutions like the CDC to become very politicized. And this is a larger pattern in the U.S. government. More and more jobs being politicized, more and more people in these jobs being on shorter, tighter leashes. More the kind of person who ends up in the job being someone who is politically pleasing to whoever happens to be in the White House. And so … the conditions for Robert Redfield being in that job were created long ago.”
“..precisely 54 children in the Land of the Free have died from COVID (according to CDC data through April 28). Given that there have been roughly 4 million confirmed COVID cases among children, this implies a survival rate of 99.999%”
In the winter of 1837, Charles Dickens published the first two chapters of what would become one of his most popular works– the story of an orphan called Oliver Twist. If you’ve never read it, the book is one of Dickens’ most damning condemnations of the poverty, crime, and child labor that dominated 19th century Britain. It was personal for Dickens; as a boy, he was forced to work long hours in a shoe polish factory for pitiful wages after his father had been hauled off to debtors’ prison. And Oliver Twist was so shocking it began a global conversation about child labor and contributed to the worldwide Children’s Rights Movement. By the early 20th century, children were starting to be viewed as more than just cheap, easily exploitable workers. Instead, western nations began to prioritize children’s well-being.
It’s been that way for generations. Then along came COVID-1984… and all the dictatorial public health measures that have accompanied it. Entire economies were locked down, borders closed, business shuttered, and basic human interactions forbidden. These restrictions have been especially damaging for children. Even to this day, more than a YEAR later, schools are still closed in many parts of the world. Millions of children simply stopped learning at the age when their minds develop more rapidly than at any other time in life. Sheepish bureaucrats hid behind Zoom classes as an adequate substitute for real learning and human interaction, though hardly a thought was given to the cost versus benefit. It’s hard to fault anyone for the decisions they made back in March or April of 2020. There was no data. And plenty of people took the most conservative approach.
But by summer 2020, there were mountains of data to support an informed decision. Consider, for example, precisely 54 children in the Land of the Free have died from COVID (according to CDC data through April 28). Given that there have been roughly 4 million confirmed COVID cases among children, this implies a survival rate of 99.999%. For kids, even the Chicken Pox is more fatal, not to mention a variety of other common illnesses ranging from the flu to strep throat. Yet the world never closed schools due to the chicken pox. Curiously, his grace, Lord Protector Anthony Fauci, noted back in 2009 during the Swine Flu epidemic that “we have already 76 children dying from the 2009 H1N1 virus, and it’s only the beginning of October.”
Yet his eminence did not demand schools close. And the CDC specifically recommended NOT closing schools. (Fauci also stated then, “you can’t isolate yourself from the rest of the world for the whole flu season. . .”) Point is, public health bureaucrats and school officials clearly didn’t conduct a basic cost/benefit analysis before closing the schools. They didn’t consider how many kids would fall behind. Or the mental health consequences of social isolation, like the higher rates of self-harm and skyrocketing calls to suicide hotlines. The only thing that mattered was a disease with a 99.999% survivability rate. Not their learning, their future, or their mental health.
Cambodia is not alone in its rapid decline since February. While the unfolding public health disaster in India dominates global headlines, a slower burning crisis is emerging across Southeast Asia’s Greater Mekong Subregion, with Thailand and Laos also witnessing a spike in cases in recent weeks and months. Once heralded as unique case studies in successfully containing the virus, seemingly immune to its most severe health effects, these three nations are now brewing outbreaks fuelled by potent strains, porous borders and public holidays. With the virus spreading on its doorstep, Vietnamese officials are anxiously preparing for what seems an inevitable arrival of cases. Though infection rates remain low in Vietnam, it now joins its neighbours in the scramble to halt the spread of Covid-19 before it’s beyond control in a region collectively home to nearly 200 million people.
Dr Jessica Manning, a researcher at the National Institutes of Health (NIH), told the Globe that B.1.1.7 has exposed many previously held myths surrounding the Mekong region’s supposed resilience to the virus. “We thought that there was this mystery to the Mekong, that maybe Southeast Asia was faring better than the rest of the world because of preexisting immunity,” said Manning, who has studied infectious diseases in Cambodia since 2017, pivoting in January last year to track Covid-19 in the Kingdom. “But with the new variants that have exploded, it’s just so much drastically worse that we no longer harbour those thoughts of Cambodians or Thais or Vietnamese having some shield related to pre-existing immunity. B.1.1.7 has just blasted through all of that.”
It’s within recent memory that Cambodia still boasted some of the best Covid-19 public health statistics globally. As of late January, the Kingdom recorded the fourth lowest cases per capita worldwide, and was also the largest country population-wise to report no fatalities of those with more than 20 cases. At that point, simple public health measures proved effective in containing the virus. “With the wild type [early] virus, Cambodia seemed to do ok with these really bread and butter public health measures, like quarantine, lockdown, schools closed, good contact tracing,” Manning said. But since that ill fated night, cases have jumped from 516 as of February 20 to 17,621 as of May 7. The B.1.1.7 variant, now Cambodia’s dominant strain, according to Kinzer and Manning, has spread with ruthless efficiency. Deaths have also begun to mount with 114 as of publishing – dispelling yet another myth around Cambodia’s resilient, youthful population.
“Her statement also preemptively warned that the “negotiations will take time given the consensus-based nature of the institution and the complexity of the issues involved” — a process that could provide drugmakers an opening to try to limit a final waiver.”
Several of President Joe Biden’s most powerful appointees and advisers have had business relationships with pharmaceutical giants lobbying the administration on COVID-19 and intellectual property issues, according to documents reviewed by The Daily Poster. Those ties — and Biden’s longtime alliance with pharmaceutical industry interests — could prove particularly relevant as drug companies now try to defang any new waiver of patent rules that might reduce their profits and facilitate the wider distribution of vaccines to COVID-afflicted countries. Last summer, Biden broke with his own legislative record and pledged to support relaxing those intellectual property rules to distribute a COVID-19 vaccine, saying it “is the only humane thing in the world to do.”
With the pandemic creating a full-fledged humanitarian crisis in India this spring, Biden’s administration on Wednesday issued a statement reiterating that general promise. “This is a global health crisis, and the extraordinary circumstances of the COVID-19 pandemic call for extraordinary measures,” said United States Trade Representative Katherine Tai in a press release. “The administration believes strongly in intellectual property protections, but in service of ending this pandemic, supports the waiver of those protections for COVID-19 vaccines.” The declaration was widely hailed by public interest groups, who feared the administration would follow past precedent and oppose any emergency action on patents.
However, Tai’s statement was narrow: It only mentioned COVID vaccines and avoided endorsing an existing, broad waiver proposed by India and South Africa which would cover “diagnostic kits, vaccines, medicines, personal protective equipment and ventilators.” Her statement also preemptively warned that the “negotiations will take time given the consensus-based nature of the institution and the complexity of the issues involved” — a process that could provide drugmakers an opening to try to limit a final waiver.
Among other things, the horror show of corruption in Ukraine, starring (but not limited to) Joe and Hunter Biden in their ceaseless quest for grift, but also featuring many of the origins of the RussiaGate hoax and its spin-offs, plus the involvement of State Department personnel such as Ambassador Marie Yovanovitch and deputy George Kent, double-plus the shady activities of George Soros and his Atlantic Council in seditious activity working hand-in-hand with the CIA’s “whistleblower” (Eric Ciaramella) to damage Mr. Trump — who was impeached for simply inquiring about what was going on in Ukraine.
Mr. Giuliani had to conduct his own investigation into all that for the obvious reason that the usual US agencies who would ordinarily investigate official misconduct were actually perpetrating it: the DOJ, FBI, CIA, and State Department. And who, at the DOJ now, might be behind the current effort to neutralize Mr. Giuliani? Try Lisa Monaco, the new Deputy Attorney General, formerly one of Barack Obama’s chief White House fixers — i.e., an attorney detailed to shutting down investigations and covering the tracks left by questionable operations — and a protégé of former CIA Director John Brennan. Is the weak and pliable AG Merrick Garland fronting for her running the DOJ now? Joe Biden is going to need a whole lot of fixin’. And, is Lisa Monaco actually still reporting to Barack Obama? He can also probably use a fix or two. Who knows what’s coming down pike? Just maybe a loaded semi driven by the nearly forgotten John Durham?
MSNBC might have made an unforced error on Wednesday scripting 10 o’clock troll Lawrence O’Donnell to diss former AG William Barr — some jive about Mr. Barr trying to mess with Special Counsel Robert Mueller’s efforts back in 2018 to nail Mr. Trump on an obstruction of justice rap. Is this the time to piss-off Mr. Barr? You have to wonder. Is it possible that the FBI concealed its possession of the Hunter Biden laptop from Mr. Barr during those 2019 days of impeachment, when Mr. Trump was attempting to mount a defense for making a phone call to Ukraine? Who might be responsible for hiding that, if it were so? By the way, it was Mr. Barr who, just before resigning in late 2020, made John Durham a Special Counsel, whose work — whatever that might be, maybe nothing at all, maybe something consequential, nobody knows — can’t be blocked by Merrick Garland (or Lisa Monaco).
The market was temporarily shaken in March 2020, as stocks plunged for about a month at the outset of the Covid-19 outbreak, but then something strange happened. Even as hundreds of thousands of lives were lost, millions of people were laid off and businesses shuttered, protests against police violence erupted across the nation in the wake of George Floyd’s murder, and the outgoing president refused to accept the outcome of the 2020 election — supposedly the market’s nightmare scenario — for weeks, the stock market soared. After the jobs report from April 2021 revealed a much shakier labor recovery might be on the horizon, major indexes hit new highs.
The disconnect between Wall Street and Main Street, between corporate CEOs and the working class, has perhaps never felt so stark. How can it be that food banks are overwhelmed while the Dow Jones Industrial Average hits an all-time high? For a year that’s been so bad, it’s been hard not to wonder how the stock market could be so good.
To the extent that there can ever be an explanation for what’s going on with the stock market, there are some straightforward financial answers here. The Federal Reserve took extraordinary measures to support financial markets and reassure investors it wouldn’t let major corporations fall apart. Congress did its part as well, pumping trillions of dollars into the economy across multiple relief bills. Turns out giving people money is good for markets, too. Tech stocks, which make up a significant portion of the S&P 500, soared. And with bond yields so low, investors didn’t really have a more lucrative place to put their money. To put it plainly, the stock market is not representative of the whole economy, much less American society. And what it is representative of did fine.
The United States added 266,000 jobs in April, according to data released by the Labor Department Friday—much worse than the 1 million job gains economists expected and far fewer than the 916,000 jobs added in March, indicating that the long-tepid labor market recovery is slowing down again even as stocks and corporate earnings rip higher. The unemployment rate ticked up to 6.1% in April, as compared to 6% in March; the metric hit a record high of 14.7% in April 2020. There are now 9.8 million unemployed people in the United States, higher than 9.7 million in March and much higher than the prepandemic level of 4 million in February 2020, the government said. Overall, the U.S. economy has added back roughly 14 million of the 22 million jobs lost at the height of pandemic uncertainty in March and April of last year.
At 3.5 million, the number of permanent job losers is still about three times prepandemic levels, and the labor force participation rate in April was little changed at 61.7%, compared to 63.4% in February 2020. According to the Labor Department, 9.4 million people reported that they were unable to work last month because their employer closed or lost business as a result of the pandemic—still a sizable portion of the labor market but down from 11.4 million in March, thanks to businesses reopening. April’s report also continued to show stark differences in unemployment by race, with minority groups such as Black Americans and Hispanics facing above-average unemployment rates of 9.7% and 7.9%, respectively.
“Obviously, the jobs report is a large disappointment . . . however, the economy is still on a recovery footing,” says Vital Knowledge Media Founder Adam Crisafulli. “Notable job gains in leisure and hospitality, other services, and local government education were partially offset by losses in temporary help services and in couriers and messengers.” The losses in temporary help services, Crisafulli says, suggest companies “may be gearing up for more permanent hires.” 16.2 million. That’s how many people are still receiving some form of government unemployment benefit—shockingly high compared to historical levels, according to weekly data released Thursday. It’s also higher than the number of unemployed Americans due to the startling number of people who’ve dropped out of the labor force because they’re no longer looking for work.
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Steven Donziger must be supported.
For millennia, Indigenous peoples in Ecuador lived prosperously with no money. But they were rich—very rich. Then Chevron came.
Here is my recent interview with journalists Jake Marquez and Maren Morgan about the human devastation caused by Chevron in Ecuador. pic.twitter.com/MmBcgh5JMt