
René Magritte Youth 1924

May 2021
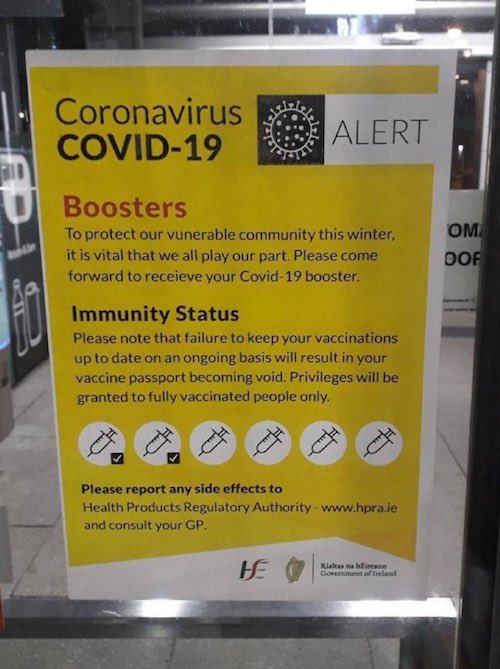
Ireland: at least 6 jabs.
We often hear people say: “Now is not the time to panic!”
But these are different times. There’s no such thing as too much panic today.
Ewan Birney is deputy director general of the European Molecular Biology Laboratory and director of EMBL’s European Bioinformatics Institute.
• Early Action Against Omicron Is Imperative (Birney)
It was only a matter of time before a new Sars-CoV-2 variant of concern emerged, requiring an urgent global response. It would seem that the Omicron variant, identified by scientists across Africa, including the National Institute for Communicable Diseases (NICD), poses the next major threat in the course of the pandemic. Early evidence from their genomic surveillance suggests that this new variant is a serious cause for concern and it is imperative that we act fast in response to this new information. The variant has also been detected in Botswana and Hong Kong, and will undoubtedly continue to arise in other territories in the coming days; travel-related cases have appeared in Belgium and Israel. Two cases of the new variant have been detected in the UK at the time of writing.
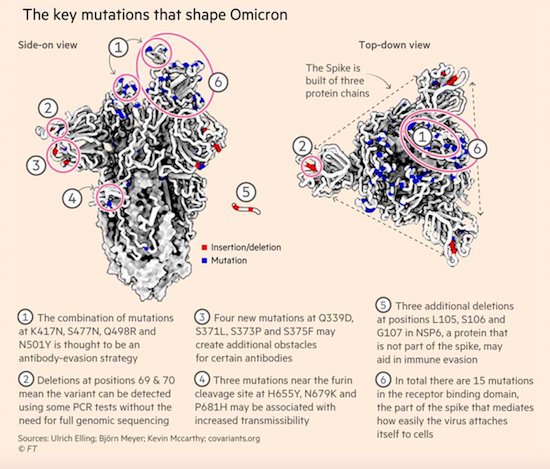
When Omicron was first detected, viral genomic experts already noted the large number of changes relative to the original Wuhan strain. Worryingly, a significant number of these mutations are linked to the spike protein, which the virus uses to infect our cells, and some of these were changes known to be responsible for either faster transmission or immune escape in other strains. However it is possible that other changes in this strain made the virus less good at transmission. It appears that the Omicron variant is on the rise. The South African researchers could be more confident of this due to a quirk in the virus also seen in the Alpha variant; there is a change that affects the readout of some of the routine PCR tests (“S-gene target failure”).
This means that the South African researchers could reprocess the routine tests they have to create an effective proxy for the rise of this variant. The strong growth inferred by proxy (albeit from a low baseline), and the sequence information we have, mean that there is a high likelihood this is either a more transmissible or immune-system evading virus, or some of both. There is not yet data to suggest that the Omicron variant increases the severity of disease or resistance to our current vaccines. This will require future laboratory investigation and continued surveillance in many countries over the coming weeks. And we should consider this potential immune-escape discovery, which was on nearly every epidemic plan, in the context of our progress: genomic sequencing identified the new variant at high speed; thanks to open data-sharing, the global scientific community was alerted to it and has sprung into action – yet again – to understand what the dangers are.
Finally, our experience and understanding of the Alpha and Delta variants make it clear that early action is far better than late response. It may turn out that this variant is not a major threat, but the consequences of not acting early could be devastating. The real heroes of this story, though, are the Botswanan and South African scientists who rapidly assembled data, delivering insightful analysis, and were open and transparent about their results.
“So are we seriously worried? No. We are concerned and we watch what’s happening. But for now we’re saying, ‘OK: there’s a whole hype out there. [We’re] not sure why.’”
• South African Medical Head: Slow-Roll the Panic Over Omicron (RS)
The variant was just discovered this week, but already you can hear the race to paint it in the worst light possible, suggesting that there was a lot to be concerned about because it was “heavily mutated,” that immunity and the vaccines might not protect against it. We saw the Dow take a huge plunge immediately after, likely in part because of thinking that this news could lead back to more government restrictions and problems. The Biden administration reacted in a chaotic fashion. First, Dr. Anthony Fauci said they weren’t going to be jumping to banning travel from affected areas and then a couple of hours later, Biden announcing there would be a ban on eight African countries starting Monday at the recommendation of Fauci.
Now obviously, the new variant was just discovered, so I don’t know how anyone can be drawing any real conclusions about it yet; they haven’t had the time to actually study it much yet. It is, of course, wise to be cautious about it. But being wise and causing panic are not the same thing. It’s important not to miss what the people who discovered it — the folks in South Africa — are saying about what they’ve seen with the variant so far. The chairwoman of the South African Medical Association called imposing the travel restrictions on the country “hasty.” Dr Angelique Coetzee said it was too early to tell what impact the variant would have. She told BBC News: “We think it is a premature decision that has been taken, I think it is a hasty decision.
“I would understand if it was two weeks later and we know much more about this viral infection that is going around, or this mutation, but for now, it is like a storm in a teacup. “We have only become aware of this viral mutation, or the new strain we are seeing, last week.” She added: “From us as medical practitioners, we picked up, last week, the different clinical pictures, we looked at the advisory committees and so far what we have seen is very mild cases. [I’m] not sure why we are all up in arms. “We know there are a lot of mutations but no-one can tell us at this stage if it means something, or if it is just going to fade away. We just don’t know.”
Coetzee told the Guardian the cases they had seen so far were extremely mild. “It’s all speculation at this stage. It may be it’s highly transmissible, but so far the cases we are seeing are extremely mild,” she said. “Maybe two weeks from now I will have a different opinion, but this is what we are seeing. So are we seriously worried? No. We are concerned and we watch what’s happening. But for now we’re saying, ‘OK: there’s a whole hype out there. [We’re] not sure why.’” Coetzee said she’d only seen it in healthy people so far, so she wasn’t sure how it would do in unhealthy people with co-morbidities. In other words, it might change and there may be causes for concern, but they’re not freaking out yet about it because they don’t have the evidence yet since it just appeared.
“Omicron variant “presents mild disease with symptoms being sore muscles and tiredness for a day or two not feeling well. […] as medical practitioners, we don’t know why so much hype is being driven” – Dr. Angelique Coetzee, Chair of SAMA
"I can promise you other countries, when they pick up a new variant, they're going to be very careful before they announce it, looking at what happened to us"
Strong words from Dr Angelique Coetzee from the South African @SAMedicalAssoc reacting to travel bans. #Omicron pic.twitter.com/SmrASoml0p
— Luxmy Gopal (@luxmy_g) November 27, 2021
“Mass vaccination has compressed the evolutionary trajectory of the virus from a few hundred years (?) down to one year.”
• My Opinion On The New African Variants (VanDenBossche)
The world may be taken by surprise but that doesn’t include us. It remains to be seen whether Omicron can outcompete Delta (to be confirmed). If that’s the case, we’re definitely not in good shape. In case of CoV, innate immunity protects the individual and the ‘herd’ (sterilizing immunity, no natural selection pressure, herd immunity) whereas adaptive immunity induced with leaky vaccines has exactly the opposite effect. THE big Q is whether such an immune escape variant could even resist naturally acquired Abs in people who recovered from C19 disease. I am, indeed, cautious and worried about ADE, even in the unvaccinated who recovered from C-19 disease as they may no longer be able to control viral infection. ADE would equal ‘enhanced virulence’. Difficult to predict. Mass vaccination has compressed the evolutionary trajectory of the virus from a few hundred years (?) down to one year. Hope that naturally primed individuals can deal with that speed.
“..while the vaccine provides temporary protection against infection, the efficacy declines below zero and then to negative efficacy territory at approximately 7 months..”
• Are We Overreacting to Omicron? (BI)
[..] governments asked us for two weeks to flatten the curve to help prepare hospitals so that they can tend to surges and other non-Covid illnesses. We as societies gave our governments 2 weeks, not 21 months. They failed to tend to the non-Covid illnesses and we locked down the healthy and well (children and young and middle aged healthy persons) while failing to properly protect the vulnerable and high-risk persons such as the elderly. We failed and it was like killing fields in our nursing homes. This failure rests on public health messaging and government. Additionally, what did our governments in the US, Canada, UK, Australia etc. do with the tax money for the hospitals and PPE etc.? Hospitals must be prepared by now. Governments have failed! Not the people. The Task Forces have failed, not the people.
These nations thought that they could stay locked down and wait for a vaccine. This is a reasonable view though I was against lockdowns as they would and did cause crushing harms on especially poor persons and children. The problem is there was an opportunity cost because the vaccine we were waiting on was suboptimally developed without the proper safety testing or assessment of effectiveness. We have data that the Pfizer vaccine loses 40% of antibodies per month, meaning in 3 months post-shot, you have low effective vaccinal immunity. We see it clearly playing out now whereby you got to tamp down spread with the draconian lockdowns, but you did it at the cost of natural immunity. That is the opportunity cost. So we spent on getting the vaccine and it cost us natural immunity and thus herd immunity.
For example, the vaccine has failed to stop infection and spread against Delta. We have research findings by Singanayagam et al. (fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts), by Chau et al. (viral loads of breakthrough Delta variant infection cases in vaccinated nurses were 251 times higher than those of cases infected with prior strains early 2020), and by Riemersma et al. (no difference in viral loads when comparing unvaccinated individuals to those who have vaccine “breakthrough” infections and if vaccinated individuals become infected with the delta variant, they may be sources of SARS-CoV-2 transmission to others) that reveal the vaccines have very suboptimal efficacy.
This situation of the vaccinated being infectious and transmitting the virus has also emerged in seminal nosocomial outbreak papers by Chau et al. (HCWs in Vietnam), the Finland hospital outbreak (spread among HCWs and patients), and the Israel hospital outbreak (spread among HCWs and patients). These studies have also revealed that the PPE and masking were essentially ineffective within the healthcare setting. All of the HCWs were double-vaccinated yet there was extensive spread to themselves and their patients.
[..] the Swedish study (retrospective with 842,974 pairs (N=1,684,958) is particularly alarming for it shows that while the vaccine provides temporary protection against infection, the efficacy declines below zero and then to negative efficacy territory at approximately 7 months, underscoring that the vaccinated are highly susceptible to infection and eventually become highly infected (more so than the unvaccinated). A further example emerges from Ireland whereby reporting suggests that the Waterford city district has the State’s highest rate of Covid-19 infections, while the county also boasts the highest rate of vaccination in the Republic (99.7% vaccinated). Reports are that the U.S. Covid-19 deaths for 2021 surpassed the deaths from 2020, leading some to state that “more people have died from COVID-19 in 2021, with most adults vaccinated and nearly all seniors), than in 2020 when nobody was vaccinated.”
A long list. These are just the vaccines.
• The Right Way To Handle The Pandemic (Kirsch)
1/ Stop the vaccines now. The current COVID vaccines kill more people than they can possibly save from COVID, even if they were 100% effective so should be taken off the market immediately. For example, the vaccine may kill 117 kids for every kid that is saved from COVID.
2/ The liability exemption is now lifted retroactively. Patients who have been harmed by the COVID vaccines can now sue the drug company for damages up to $100M per case of fatality or disability.
3/ Every post-vaccination ailment, affliction and death appearing within 4 weeks of vaccination that appears at a rate of 10X or more vs. baseline should be attributed to the vaccine unless and until proven otherwise, by irrefutable evidence, with costs of all diagnostic procedures to be born by the pharmaceutical manufacturer.
4/ For future approved vaccines, informed consent provide shall include any and all symptoms that are elevated in VAERS by 10X or more over “baseline” reporting rates.
5/ For future approved vaccines, require autopsies for anyone who dies within 2 weeks of getting the vaccine. The autopsy reports should be posted in a public database with Names and other PHI related data redacted
6/ Failure to file a VAERS report for anyone who dies within 30 days of COVID vaccination shall be liable to a fine of $100,000 per incident.
“Note that on the evidence to date there is no reason to believe this “variant” is either more-dangerous or more transmissible. SA had a surge in cases at the exact same time last year. It’s called “seasonality” and its real. It’s why we have a “flu season.”
• Only Two Things Are Infinite…. (Denninger)
This “variant” has been found all over the world already. Therefore its already everywhere. Locking down travel after it is already in your nation is stupid and does nothing. The variant is either going to become dominant or it will not. You cannot alter that course once it gets to you — and no matter where you are it already has. This “variant” has no evidence of being more-deadly; it may in fact be less-so. Indeed that is the natural mutational pattern coronaviruses follow over time. There is no evidence in the form, for example, of higher hospital admissions, ICU utilization and death in those in which this variant has been detected. In other words thus far all the scaremongering has been based on….. exactly nothing as there are no facts currently in evidence to support such fear.
The vaccines clearly do not work. International travel has been vaccinated-only everywhere for quite some time. So the person(s) who brought the virus into your nation with this “variant” were vaccinated. The market, of course, responded to this news by spiking the vaccine companies, specifically Moderna. You have to wonder what sort of stupidity would drive someone to consider a firm that has one product which clearly did not work a “buy” in a situation like this. Mass psychosis is the only reasonable explanation. Lockdowns and constraints clearly do not work either. The virus mutated because that’s what viruses do, and specifically coronaviruses do this all the time. It’s common.
Further, vaccinating into an outbreak promotes vaccine-resistant strains because that’s just how natural selection works. You want the opposite but you can’t get there from here by vaccinating people while an outbreak is going on so the better option is to focus on early treatments and even prophylaxis which does not place immune pressure on the virus to evade your jabs. Meanwhile we the evidence continues to mount that prior infection confers better resistance than vaccines. Perfect immunity? No. But much better immunity and, to three nines, perfect protection against critical illness and death.
[..] Only infection has ever conferred critical and fatal outcome protection with coronaviruses through history. There are no exceptions. Not only have all previous attempts ended in failure several have resulted in vaccine-enhanced disease ripping through the vaccinated test subjects on re-challenge with several of those trials ending in the death of all or nearly all test subjects — which were fortunately animals and not humans. This time around we have performed a mass experiment with zero evidence over a period of years to demonstrate that what has happened 100% of the time in the past will not happen again. It appears we’re losing that bet — a loss that, on the basis of history, we had every reason to believe would happen and yet instead of every single firm manufacturing this crap being an instant zero several are being rewarded. What the hell sort of rampant, outrageous stupidity is that?
While the data is not yet in there is reason to believe, given the mutations described in this newest “variant”, that the vaccinated may be ****ed as the mutations may confer full evasion and yet the binding antibodies you get from being jabbed are still there. If that pans out here comes the exact same thing that has repeatedly happened with coronavirus vaccine attempts except this time we were dumb enough to mass-vaccinate humans rather than a handful of cats. Note that on the evidence to date there is no reason to believe this “variant” is either more-dangerous or more transmissible. SA had a surge in cases at the exact same time last year. It’s called “seasonality” and its real. It’s why we have a “flu season.”
The confluence of mutations does raise questions though, including the possibility that our “best friends” are angling for the very scenario I put forward about a year ago — which you’d better pray is wrong, by the way, although it’ll be a while before we know. Before you poo-poo this note that there are reports the closest match to any known sequenced Covid-19 virus date to April of 2020. I have not yet personally verified this, but if its true then it is wildly improbable that an “in the wild” mutational pattern of this sort occuring by natural means would have escaped surveillance. Incidentally if you got jabbed there’s not a damn thing you can do about it if that turns out to be the case.
Steve Kirsch makes multi-million bets all the time, but puts up a paywall?!
• 45% of Deaths After Covid Vaccination Happen In The First 2 Weeks (Kirsch)
My friend Albert Benavides (aka WelcomeTheEagle88) did a quick analysis for me on the deaths reported after vaccination in VAERS. 45% of all reported deaths happened within two weeks after vaccination. Peter Schirmacher, one of the world’s top pathologists, said that 30% to 40% of people who died within 2 weeks after vaccination died were killed by the vaccine. His results were replicated by other German pathologists (since no US pathologist would dare accuse the vaccine of causing death or they would be immediately fired).
So taking a very conservative view that VAERS is 100% reported (so only a total of 8664 deaths), then 44% of 8664 = within 2 weeks = 3812 killed in the first two weeks. If just 30% was caused by the vaccines, then that is 1,143 people killed by the vaccine at a minimum. For 230M vaccinated, then that is 4.9 deaths per million minimum killed by the vaccine. This means these vaccines are at least 5X deadlier than the smallpox vaccine which we pointed out is deemed to be too unsafe to use. Note that this estimate assumes that only the deaths in the first two weeks are caused by the vaccine and assumes after 2 weeks all the excess deaths we caused by something else. Note: The actual number killed by the vaccines is at least 150K (estimated 8 different ways), but we’re trying to be as conservative as possible here giving any critics nothing to complain about.
Here are the % of total deaths for each week for the first 5 weeks:
1/ 33.6% meaning that in the first week, 33.6% of all the vaccine related deaths happened in the first week
2/ 10.97% in the second week, so now we’ve killed nearly 45% of all the deaths
3/ 8.4%
4/ 6.04%
5/ 4.19% by the fifth week out, 63% of all deaths have happened
Don’t.
As a father of a young child, I am pressured to get my daughter vaccinated for COVID-19. And like many Americans, I have concerns about giving my six-year-old a new vaccine that was not tested on humans until last year, and that has been approved only for “emergency use” in kids. The feverish hype by government officials, mainstream media outlets, and Big Pharma, and the systematic demonization and censorship of public figures who raise questions about the campaign, provide further cause for concern. This year, Pfizer has banked on selling 115 million pediatric doses to the U.S. government and expects to earn $36 billion in vaccine revenue. Congress is so in the pocket of Big Pharma that it’s against the law for our government to negotiate bulk pricing for drugs, meaning taxpayers must pay retail.
Corporate news and entertainment programs are routinely sponsored by Pfizer, which spent $55 million on social media advertising in 2020. Even late night comedians like Jimmy Kimmel, who has called for denying ICU beds to unvaccinated people, have been paid by Big Pharma to promote the COVID-19 vaccine. It is thus not surprising that most of the information reported in the press about vaccine safety and efficacy appears to come directly from Pfizer press releases. This recent headline from NBC News is typical: “Pfizer says its Covid vaccine is safe and effective for children ages 5 to 11.” Moreover, by not advertising their vaccines by name, Pfizer-BioNTech and other drugmakers are not obliged, under current FDA regulations, to list the risks and side effects of the vaccine.
Most Americans are vaguely aware that COVID vaccines carry some potential risks, such as heart inflammation, known as myocarditis, seen most often in young males. But no actual data from the vaccine trials has been provided to the public. After promising “full transparency” with regard to COVID-19 vaccines, the FDA recently went to court to resist a FOIA request seeking the data it relied on to license the Pfizer COVID-19 vaccine, declaring that it would not release the data in full until the year 2076—not exactly a confidence-building measure.
Also troubling is a recent report in the British Medical Journal, a peer-reviewed medical publication, which found that the research company used by Pfizer falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events reported in Pfizer’s pivotal phase III trial. The whistleblower, Brook Jackson, repeatedly notified her bosses of these problems, then e-mailed a complaint to the FDA and was fired that same day. If this scandal was ever mentioned in the corporate press, it was with a headline like this from CBS News: “Report questioning Pfizer trial shouldn’t undermine confidence in vaccines.”
“The checkpoints are essentially gateways where QR codes are being scanned from the cell phones of the compliant vaccinated citizen. Yes comrades, there’s an App for that.”
• Think Carefully About Accepting The Concept of Vaccine Passports (CTH)
As the architects of the Build Back Better society assist you in creating easier ways to show your vaccinated and compliant status, perhaps it is prudent to pause and think about the discussions that take place behind the opaque glass doors. Right now, as you are reading this, under the guise of enhancing your safety, the U.S. federal government is in discussions with multinational corporations and employers of citizens to create a more efficient process for you to register your vaccine compliance. You may know their conversation under the terminology of a COVID passport. The current goal is to make a system for you to show your authorized work status; which, as you know, is based on your obedience to a mandated vaccine.
Beta tests are being conducted in various nations, each with different perspectives and constitutional limitations based on pesky archaic rules and laws that govern freedom. For the western, or for lack of a better word ‘democratic‘ outlook, Australia is leading the way with their technological system of vaccination check points and registered state/national vaccination status tied to your registration identification. The checkpoints are essentially gateways where QR codes are being scanned from the cell phones of the compliant vaccinated citizen. Yes comrades, there’s an App for that. Currently the vaccine status scans are registered by happy compliance workers, greeters at the entry to the business or venue. Indeed, the WalMart greeter has a new gadget to scan your phone prior to allowing you custody of a shopping cart.

Remember: Fauci and Birx destroyed Atlas.
• A President Betrayed by Bureaucrats: Scott Atlas’s Masterpiece on Covid (Tucker)
I’m a voracious reader of Covid books but nothing could have prepared me for Scott Atlas’s A Plague Upon Our House, a full and mind-blowing account of the famed scientist’s personal experience with the Covid era and a luridly detailed account of his time at the White House. The book is hot fire, from page one to the last, and will permanently affect your view of not only this pandemic and the policy response but also the workings of public health in general. Atlas’s book has exposed a scandal for the ages. It is enormously valuable because it fully blows up what seems to be an emerging fake story involving a supposedly Covid-denying president who did nothing vs. heroic scientists in the White House who urged compulsory mitigating measures consistent with prevailing scientific opinion. Not one word of that is true. Atlas’s book, I hope, makes it impossible to tell such tall tales without embarrassment.
Anyone who tells you this fictional story (including Deborah Birx) deserves to have this highly credible treatise tossed in his direction. The book is about the war between real science (and genuine public health), with Atlas as the voice for reason both before and during his time in the White House, vs. the enactment of brutal policies that never stood any chance of controlling the virus while causing tremendous damage to the people, to human liberty, to children in particular, but also to billions of people around the world. For the reader, the author is our proxy, a reasonable and blunt man trapped in a world of lies, duplicity, backstabbing, opportunism, and fake science. He did his best but could not prevail against a powerful machine that cares nothing for facts, much less outcomes.
If you have heretofore believed that science drives pandemic public policy, this book will shock you. Atlas’s recounting of the unbearably poor thinking on the part of government-based “infectious disease experts” will make your jaw drop (thinking, for example, of Birx’s off-the-cuff theorizing about the relationship between masking and controlling case spreads). Throughout the book, Atlas points to the enormous cost of the machinery of lockdowns, the preferred method of Anthony Fauci and Deborah Birx: missed cancer screenings, missed surgeries, nearly two years of educational losses, bankrupted small business, depression and drug overdoses, overall citizen demoralization, violations of religious freedom, all while public health massively neglected the actual at-risk population in long-term care facilities.
Essentially, they were willing to dismantle everything we called civilization in the name of bludgeoning one pathogen without regard to the consequences. The fake science of population-wide “models” drove policy instead of following the known information about risk profiles. “The one unusual feature of this virus was the fact that children had an extraordinarily low risk,” writes Atlas. “Yet this positive and reassuring news was never emphasized. Instead, with total disregard of the evidence of selective risk consistent with other respiratory viruses, public health officials recommended draconian isolation of everyone.”
Why use the word “mistakes”? Call a spade a spade.
• “A Lot of Mistakes”: The Guardian and Julian Assange (MPN)
On September 21, 2018, the Guardian published a bombshell report entitled “Revealed: Russia’s secret plan to help Julian Assange escape from UK.” The story detailed an alleged conspiracy between Russian diplomats and WikiLeaks to illicitly smuggle Assange out of the Ecuadorian Embassy in London. During the months before publication, Guardian correspondent Stephanie Kirchgaessner seemed eager to connect Assange to a Russian plot to escape the embassy. On July 12, 2018, Kirchgaessner wrote to a source at UC Global, the private security company hired by the Ecuadorian government to protect Assange and its embassy in London: “We heard that the Russians wanted to help Assange and maybe get him a diplomatic visa. This was last year. But then the plan was rejected. By the Russians or by Assange? Why? Can you help? Do you know?”
On August 30, 2018, three weeks before publication, Kirchgaessner wrote again: “Hello. I am trying you again. I want to write a story about the discussions last year to get JA out of the embassy. The talks that happened with the Russians. Can I send you some questions?” When the article was eventually published, the authors — Kirchgaessner, Dan Collyns, and Luke Harding — claimed that “Russian diplomats held secret talks in London … with people close to Julian Assange to assess whether they could help him flee the UK” in late 2017. Though it was acknowledged that “details of the Assange escape plan are sketchy,” the authors used two unnamed sources to assert that Fidel Narváez, the former consul at the Ecuadorian Embassy, “served as a point of contact with Moscow.”
The story appeared to add weight to the “Russiagate” narrative – the belief that the Donald Trump campaign colluded with Russia to subvert the 2016 U.S. presidential election, with help from WikiLeaks. The authors noted that the alleged escape plan “raises new questions about Assange’s ties to the Kremlin.” Two individuals with first-hand knowledge of events reject the Guardian’s story, however, and provide details about what really happened in late 2017 when Assange tried to leave the embassy. In an exclusive interview, Aitor Martinez, a lawyer who oversaw Ecuador’s effort to grant Assange diplomatic protection, explained that plans were drawn up to appoint Assange as an Ecuadorian diplomat and transport him to a third country. That way, Assange could legally leave the Ecuadorian Embassy in London, where he was subject to arbitrary detention and where his health was declining.
Martinez drew up a list of countries that Ecuador should approach: China, Serbia, Greece, Bolivia, Venezuela or Cuba, noting: Of course, they were the countries that don’t have good relations with the U.S. and could accept the appointment. Russia was never, ever on that list. There was a huge conspiracy theory in the U.S. with Russiagate; it didn’t make sense. So those were the countries.” Martinez continued: It took two or three weeks and we didn’t get any answer from the Ministry of Foreign Affairs. And suddenly the Ministry said that they had appointed him to Russia.” Foreign Minister María Fernanda Espinosa’s cousin worked at the Ecuadorian Embassy in Moscow and, through this cousin, she concocted a plan to appoint Assange to the one country that was the subject of mass-media hysteria. “Julian and all of us at the legal team refused this appointment,” Martinez explained. “We said, ‘that’s crazy, what are you talking about?’ We refused.”
Support the Automatic Earth in virustime; donate with Paypal, Bitcoin and Patreon.
