
Doc Robinson
Forum Replies Created
-
AuthorPosts
-
Doc Robinson
ParticipantIlargi, this is related to your question. Primaquine (not chloroquine) appears to be the drug of choice to fight malaria. Primaquine also is problematic for G6PD-deficient patients. “In six decades of primaquine use in approximately 200 million people, 14 deaths have been reported.”
“G6PD deficiency provides great protection from malaria infection, especially for falciparum infections. On the other hand, G6PD deficiency has been recently demonstrated to cause serious problems in fighting against malaria. Primaquine, which is the only drug currently used in the treatment of Plasmodium infections leads to severe hemolysis in G6PD-deficient patients. This drug may even cause death in G6PD-deficient patients”
https://www.intechopen.com/books/dehydrogenases/glucose-6-phosphate-dehydrogenase-deficiency-and-malaria-a-method-to-detect-primaquine-induced-hemolPrimaquine is the only generally available anti-malarial that prevents relapse in vivax and ovale malaria, and the only potent gametocytocide in falciparum malaria. Primaquine becomes increasingly important as malaria-endemic countries move towards elimination, and although it is widely recommended, it is commonly not given to malaria patients because of haemolytic toxicity in subjects who are glucose-6-phosphate dehydrogenase (G6PD) deficient (gene frequency typically 3-30% in malaria endemic areas; >180 different genetic variants).In six decades of primaquine use in approximately 200 million people, 14 deaths have been reported. Confining the estimate to reports with known denominators gives an estimated mortality of one in 621,428 (upper 95% CI: one in 407,807). All but one death followed multiple dosing to prevent vivax malaria relapse. Review of dose-response relationships and clinical trials of primaquine in G6PD deficiency suggests that the currently recommended WHO single low dose (0.25 mg base/kg) to block falciparum malaria transmission confers a very low risk of haemolytic toxicity.”
https://malariajournal.biomedcentral.com/articles/10.1186/1475-2875-13-418ParticipantI’m not an MD, but I presented some evidence (in an earlier comment) that counters those OffGuardian claims about hydroxychloroquine and African Americans.
That OffGuardian article was based on this assertion:
“I looked at the drugs that can cause severe hemolysis in G6PD deficiency and got really scared. One of the substances that is called very dangerous in all forms of this enzyme deficiency is the anti-malarial drug hydroxychloroquine (HCQ).”A quick search for evidence indicated that this assertion is false.
There is evidently a related problem with Chloroquine (CQ), but not with Hydroxychloroquine (HCQ).“One drug commonly associated with hemolytic anemia in G6PD deficiency is … chloroquine.
Should this be a concern in the present debate over treating COVID-19 patients? In my opinion, yes. G6PD deficiency is rather common; in fact, it is the second most common human enzyme defect, affecting some 400 million people worldwide. It affects 1 in 10 African-American males in the U.S…Given the challenges of knowing who may or may not have G6PD deficiency, it would seem prudent not to use chloroquine to treat COVID-19 patients who may be at risk for this genetic condition. The last thing they need is to have a serious respiratory disease compounded by hemolytic anemia, resulting in further loss of oxygenation.
Hydroxychloroquine, on the other hand, does not induce hemolytic anemia in people with G6PD deficiency despite the molecular similarity to chloroquine. It has shown effectiveness in inhibiting the pandemic coronavirus during in vitro testing.”
Chloroquine Is Not a Harmless Panacea for COVID-19
— There’s a real safety concern with malaria drug
by Dan J. Vick MD, DHA, MBA, CPE March 23, 2020
https://www.medpagetoday.com/infectiousdisease/covid19/85552Is Hydroxychloroquine Safe for Patients with G6PD Deficiency?
There is no data to support the withholding of hydroxychloroquine (HCQ) therapy among African American patients with glucose-6-phosphate dehydrogenase (G6PD), according to the results of a recent review… “This is the largest study to date evaluating G6PD deficiency with concurrent use of HCQ,” the researchers concluded. “These data do not support routine G6PD level measurement or withholding HCQ therapy among African American patients with G6PD deficiency.”
https://www.consultant360.com/exclusives/hydroxychloroquine-safe-patients-g6pd-deficiency
ParticipantCoronavirus Deadliest In New York City’s Black And Latino Neighborhoods (R.)
Vitamin D deficiency may play a role.
Vitamin D deficiency is more common among African Americans (AAs) than among European Americans (EAs), and epidemiologic evidence links vitamin D status to many health outcomes… Vitamin D deficiency is common even among AAs who live in sunlight intense southern and southwestern states or who have higher dietary vitamin D intake than the longstanding recommended daily allowance (≥400 IU/day)
Common vitamin D pathway gene variants reveal contrasting effects on serum vitamin D levels in African Americans and European Americans
https://link.springer.com/article/10.1007/s00439-014-1472-yParticipantIn July 2019, the Virginia Department of Health issued a warning about an increase in respiratory illnesses in multiple regions “across the Commonwealth”.
“Since the end of flu season in May, the Virginia Department of Health has received increased reports of respiratory (breathing) illness across the Commonwealth greater than observed in previous summers. Most of the reports have occurred among older adults and those with chronic medical conditions in assisted living and long-term care facilities.”
ParticipantThe CDC tested 17 samples, but “had not been able to identify” the cause of the outbreak, and noted that “several” samples tested positive for rhinovirus.
“Working with the county health department along with the Virginia Department of Health, the U.S. Centers for Disease Control and Prevention tested 17 samples taken from ill residents, but as of July 19, the agency had not been able to identify a specific cause for the sudden uptick in respiratory illness from either that initial testing or additional laboratory testing.
CDC test results uncovered several bacteria known to “colonize” the nose and throat but may not be the cause of infection, and several specimens tested positive rhinovirus, the respiratory virus most frequently found in humans and the main source of the common cold, according to the Fairfax County Health Department.”
ParticipantAfter at least 2 weeks of testing in July 2019, the CDC reportedly didn’t identify the cause of the outbreak, “despite extensive testing of multiple specimens”. A few days later, rhinovirus was indicated when the county health department wrapped up its investigation. It took that long for the CDC to identify a rhinovirus as the cause?
Participant@ John Day
“cases of a previously unknown and serious respiratory illness appeared at a retirement village on the western outskirts of the capital in July 2019”Local news story, July 12, 2019:
The symptoms usually start with a cough. In less than 2 weeks, a mystery virus at Springfield’s Greenspring Retirement Community has gotten 55 residents sick. Twenty have been hospitalized — some with pneumonia — and two people have died... …Dr. Schwartz says the community is taking proper steps and thoroughly cleaning the facility while Inova Health and the Center for Disease Control and Prevention work to figure out what kind of a virus this is and how it is spreading. “These panels have looked for several of the most common pathogens and they have been negative so far,” said Dr. Schwartz.
https://wjla.com/news/local/mystery-virus-greenspring-retirement-cdc-vaWashington Post, July 19:
Third person has died after respiratory illness outbreak at Greenspring Village, Fairfax officials say
CDC has tested 17 samples but has so far failed to identify the cause.
https://www.washingtonpost.com/dc-md-va/2019/07/17/third-person-has-died-after-respiratory-illness-outbreak-greenspring-village-fairfax-officials-say/From the official website for the Health Department at Fairfield County:
July 11 update
“A specific cause has not yet been identified but additional tests are being done by the Virginia Department of Health and Inova Health System.”July 15 update
“No cause for the illnesses has yet been identified, but the Health Department is working with the Virginia Department of Health and the Centers for Disease Control and Prevention (CDC) to conduct testing for viruses and bacteria that may cause respiratory illness.”July 16 update
“Results of testing by the Centers for Disease Control and Prevention (CDC) are still pending”July 17 update
“CDC tested 17 specimens from ill Greenspring residents. No cause for the outbreak was identified.“July 19 update
“Additional laboratory testing from CDC has not identified a specific cause for the increase in respiratory illness.”July 26 update
“Despite extensive testing of multiple specimens, no specific pathogen was identified as the cause of the outbreak.”July 29 (final update)
“Results of earlier testing submitted to the Centers for Disease Control and Prevention indicated rhinovirus, a virus that causes the common cold.“https://www.fairfaxcounty.gov/health/outbreak-investigation-assisted-living-facility-springfield
ParticipantJohn Day: Why is China not giving out vitamin-D like free condoms in New Orleans?
Excellent question.
“Vitamin D deficiency is prevalent among all age groups in China”
The High Prevalence of Hypovitaminosis D in China
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4554140/“Vitamin D inadequacy is common among the elderly, especially within the Asian population.”
Vitamin D status among the elderly Chinese population
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5237548/ParticipantHow ‘Overreaction’ Made Vietnam A Virus Success (BBC)
With the benefit of hindsight, some ‘overreactions’ can still look like overreactions, while some others can end up looking like under-reactions. That’s the thing about uncertainty and limited information. Precautions, based on the best information available at the time, can later be seen as mistakes, when the situation becomes more clear. Rational caution could retrospectively be construed as irrational fear.
If a family pays for 12 months of auto insurance, but is not involved in any car accidents during the entire year (and they are not stopped by the police during that year), then was the money wasted? Was it a mistake for them to pay for car insurance that year? Were they too fearful about the small possibility of being in a car crash?
ParticipantFrom an article highly recommended for those who are trying to keep an open, rational mind:
Our narratives of COVID-19 are all lies.
They are lies of a particular sort, political narratives that have a nugget of truth within them, but are told with bad intent. They are told this way because it works. Because the nugget of truth hides a deeper, unpleasant truth. And a Big Lie.Some are narratives of the political left. Some are narratives of the political right.
They are all narratives of betrayal, meaning that they seek to excuse or promote policies designed for institutional advantage rather than the common good.
How do you recognize a political narrative of betrayal?
It’s always based on a model…
Model-driven Narrative #3
Flatten the Curve!Political goal: COVID-19 threat maximization.
Truth nugget: Lockdowns prevent a surge in cases which can overwhelm the healthcare system.
Deep Truth nugget: When we’ve got everyone freaked out about staying alive, there’s no end to the crazy authoritarian stuff we can get away with.
Big Lie: We can get R-0 down to zero.
Policy prescription: You’ll find these ankle monitors to be surprisingly light and comfortable to wear!
Embedded model: Laughably inaccurate models of COVID-19 deaths, malleable enough to serve the political aspirations of both the White House and their opponents.…Today, “Flatten the Curve!” has become the narrative rationale for a range of extraordinary executive actions – on both the left AND the right – that would make Lincoln blush. This is the narrative that will propel the Surveillance State into a permanent feature of American life. This is the narrative that will propel the final transformation of capital markets into a political utility. This is the narrative that will propel us into a war with China. If we let it.
(This article was also linked by Ilargi, above.)
https://www.epsilontheory.com/a-truth-thats-told-with-bad-intent/ParticipantHuskynut: “It’s possible (and sensible) to hold two truths concurrently – that sensible precautions against controlling excess spread and deaths from Covid are essential. And that most Western governments have done a pretty average job in terms of analysing and responding to the data as it arises. There’s been far too little transparent debate, far too much capture by industry experts and consequent herd thinking. Ginormous, earth-shaking decisions such as blanket suspension of civil liberties for arbitrary periods of time, and vast, vast debts being rung up with negligible oversight.”
I would agree with this. And I would readily admit that I don’t know what the best approach would be. Covid-19 falls somewhere between scary Ebola and ho-hum seasonal flu.
Participantkimyo99, I found this info which might be helpful, in addition to whatever John Day may recommend.
“Breathing exercises are actively encouraged post operatively and could probably be advised to recovering COVID-19 patients as well. If we look at the types of breathing exercises that have been used after major surgeries, no difference in benefit has been found when using an incentive spirometer – essentially a game-like device to blow a ball a round – or simple deep breathing exercises5 with either approach giving a benefit to the patient in recovery. Thus, it would be quite reasonable for similar advice to be extended to the post coronavirus patients, in the hope of producing a short term benefit in improvement of their breathing. Many surgical departments have freely available breathing exercises on their patient pages which can easily be accessed by patients6.
“As for nutritional support in recovery, simple advice ensuring consumption of five fruits and veg a day should be advised, along with increased intake of high quality protein to provide resources for the repair of muscles which will have been taxed considerably during the course of the COVID19 symptoms. As the focus in the post-acute phase is going to be on the recovery of a patient’s respiratory function, cessation of smoking should be encouraged along with avoidance of ibuprofen where possible.”
https://www.sciencemediacentre.org/expert-comment-on-treatment-and-recovery-post-covid-infection/
Participant“hydroxychloroquine and zinc early is key. Unless it is contraindicated by the specific genetic background of the individual.”
That article yesterday was based on this assertion:
“I looked at the drugs that can cause severe hemolysis in G6PD deficiency and got really scared. One of the substances that is called very dangerous in all forms of this enzyme deficiency is the anti-malarial drug hydroxychloroquine (HCQ).”A quick search for evidence indicated that this assertion is false.
There is evidently a related problem with Chloroquine (CQ), but not with Hydroxychloroquine (HCQ).One drug commonly associated with hemolytic anemia in G6PD deficiency is … chloroquine.
Should this be a concern in the present debate over treating COVID-19 patients? In my opinion, yes. G6PD deficiency is rather common; in fact, it is the second most common human enzyme defect, affecting some 400 million people worldwide. It affects 1 in 10 African-American males in the U.S…
Given the challenges of knowing who may or may not have G6PD deficiency, it would seem prudent not to use chloroquine to treat COVID-19 patients who may be at risk for this genetic condition. The last thing they need is to have a serious respiratory disease compounded by hemolytic anemia, resulting in further loss of oxygenation.
Hydroxychloroquine, on the other hand, does not induce hemolytic anemia in people with G6PD deficiency despite the molecular similarity to chloroquine. It has shown effectiveness in inhibiting the pandemic coronavirus during in vitro testing.
Chloroquine Is Not a Harmless Panacea for COVID-19
— There’s a real safety concern with malaria drug
by Dan J. Vick MD, DHA, MBA, CPE March 23, 2020
https://www.medpagetoday.com/infectiousdisease/covid19/85552Is Hydroxychloroquine Safe for Patients with G6PD Deficiency?
There is no data to support the withholding of hydroxychloroquine (HCQ) therapy among African American patients with glucose-6-phosphate dehydrogenase (G6PD), according to the results of a recent review.
The researchers conducted a retrospective chart review that included 275 patients with a measured G6PD and HCQ usage (84% of patients were female and 46% were African American).
Of the 275 patients, 32% were diagnosed with lupus, 29% with rheumatoid arthritis, and 14% with inflammatory arthritis. Only 4% of patients were G6PD deficient, all of which were African American.
Overall, there were no incidents of hemolysis reported in over 700 months of HCQ exposure among the 11 G6PD-deficient patients. Two G6PD-deficient patients experienced hemolysis during severe lupus flares that occurred while not taking HCQ.
“This is the largest study to date evaluating G6PD deficiency with concurrent use of HCQ,” the researchers concluded. “These data do not support routine G6PD level measurement or withholding HCQ therapy among African American patients with G6PD deficiency.”
https://www.consultant360.com/exclusives/hydroxychloroquine-safe-patients-g6pd-deficiency
ParticipantPrices overall went down significantly, but food prices went up significantly.
The BLS reports consumer prices are in negative territory for the month with both the CPI and core CPI in negative territory.
The Consumer Price Index for All Urban Consumers (CPI-U) declined 0.8 percent in April on a seasonally adjusted basis, the largest monthly decline since December 2008.
Food indexes rose in April, with the index for food at home posting its largest monthly increase since February 1974.
https://www.thestreet.com/mishtalk/economics/cpi-and-core-cpi-in-rare-negative-territory
Participant@anticlimactic, this latest data from New York City might be helpful.
NYC COVID-19 Deaths Among Confirmed Cases
Age Group
0 to 17 — nearly 0%
18 to 44 — 4%
45 to 64 — 22%
65 to 74 — 25%
75 and over — 49%(75% had known underlying conditions.)
https://www1.nyc.gov/assets/doh/downloads/pdf/imm/covid-19-daily-data-summary-deaths-05102020-1.pdf
Participant“In the Winter of 2014/15 [in the UK] there was a severe form of the common flu. 40,000 people died.”
That sounded interesting, so I looked it up. The 40,000+ deaths figure is not the number of flu deaths, and it’s not the excess mortality compared to previous years, it’s actually the “excess winter mortality, the difference between the average number of deaths over the winter [December through March] and the rest of the year [the non-winter months]”.
“In common with other countries, in England and Wales more people die in the winter than in the summer… There were an estimated 43,900 excess winter deaths (EWDs) in England and Wales in 2014/15, representing 27% more deaths in the winter period, compared with the non-winter period… Respiratory diseases were the underlying cause of death in more than a third [not 100%] of all excess winter deaths in 2014/15.”
To look at excess deaths during a flu season, or an epidemic or pandemic, the number of deaths should be compared to what is “normal” for that time of year (e.g. the 5-year average).
For 2014/2015:
“Daily deaths peaked on 1 January 2015, 35% higher than the five-year average“For 2019/2020:
Weekly deaths are now about 100% higher than the five-year averageParticipantStill too early to tell, but some numbers from yesterday’s Debt Rattle indicate that Sweden’s approach might not result in much economic benefit, compared to neighboring countries having official lockdowns. Sweden’s GDP is forecast to shrink more than Denmark’s.
Spring 2020 GDP growth forecast for the EU (as of May 06, 2020)
Finland -6.3%
Sweden -6.1%
Denmark -5.9%ParticipantThe Financial Times graph (above) shows 61% excess deaths (during the outbreak) for this calendar year (so far), compared to the same period in recent years.
The chart posted by Dr D shows 20 weeks of the 2019/2020 season (including only the first 4 weeks of deaths from Covid-19), compared to 20 weeks of deaths from the 5 worst flu seasons in the past 25 years.
Participant“The chart is saying the deaths this year aren’t really that off trend from other years.”
That chart is actually misleading, since although it’s comparing the same 20-week stretches of the six worst years in the past 25 years (including this season so far), the 2020 data only includes 4 weeks where there are any deaths from Covid-19. The Covid-19 deaths are still happening at a significant rate, so it’s too early to make an apples-to-apples comparison.
Here’s a better indication of the situation, with the appearance of Covid-19 deaths causing the total deaths to jump above the 5-year average, climbing to about 200% of the 5-year average (in recent weeks):
https://www.ons.gov.uk/visualisations/dvc812/fig1/line/index.html
ParticipantOkay, forget Snopes, here’s an article from 2011 with some background regarding the firing and subsequent arrest of Judy Mikovits.
In 2010, we published a story about an amazing scientific finding that had caused enormous waves in medicine. Researchers reported finding a link between a retrovirus called XMRV and chronic fatigue syndrome, a frustrating disorder with no proven explanation and no cure. The findings were reported in a paper in one of the most prestigious journals in the world – Science.
What grabbed our attention was what some of the scientists involved with the paper did after its publication in 2009. The lead researcher, Judy Mikovits, began making sweeping unsupported statements about the finding, including tying XMRV to autism without publishing any data to support that statement. Some CFS patients began taking potent antiretroviral drugs meant to treat HIV.
The problem with all of this was that in science, findings don’t mean much until they are replicated. Scientists are often wrong, even when they publish in prestigious journals. And in this case, soon after the Science paper came out, independent teams were unable to replicate the findings. They could not find evidence of XMRV in the blood of CFS patients – or anyone else for that matter. Talk of contamination – a not-unheard-of problem in virology labs – arose.
Mikovits adamantly denied contamination had anything to do with her results.
[Trine has written about this back-and-forth on Trib Nation before, and you may have joined her for a livechat on the topic in December 2010. We covered a lot of ground in that discussion. — Eds.]
Recently, we reported that the journal Science had launched an investigation into whether a figure in Mikovits’ 2009 paper had been manipulated. Soon after, Mikovits was fired from the Whittemore Peterson Institute for Neuro-Immune Diseases, the Reno, Nev., non-profit created by the parents of a daughter with CFS. Last week, WPI filed a civil lawsuit against Mikovits, accusing her of taking lab notebooks and a computer that belonged to WPI.
On Nov. 18, Mikovits was arrested in Ventura, Calif., as a fugitive.
The University of Nevada, Reno police issued an arrest warrant listing two felony charges: possession of stolen property and unlawful taking of computer data, equipment, supplies or other computer related property. Mikovits will be arraigned Tuesday afternoon in California.
ParticipantSnopes provided this background regarding the firing and subsequent arrest of researcher Judy MIkovits.
In 2009, biologist Judy Mikovits, who was then the research director of the Chronic Fatigue Syndrome-focused Whittemore Peterson Institute (WPI), published a paper on what she and many others thought to be a major scientific breakthrough in the prestigious journal Science. Her team alleged to have demonstrated an association between a newly discovered retrovirus called “xenotropic murine leukemia virus-related virus” (XMRV) and the poorly understood condition known as Chronic Fatigue Syndrome (CFS), suggesting a potential viral cause for CFS.
The paper received substantial international coverage. However, as with so many other potentially groundbreaking studies, nobody — including many of the same researchers involved with the original study — was able to replicate its results. Numerous attempts failed to replicate the study, and the research itself came under increasing scrutiny for sloppy methods and its reliance on misleading or manufactured figures.
On 1 July 2011, Science’s editors issued a “statement of concern” about the paper. On 14 October 2011, the authors issued a partial retraction of their paper that touched on issues with some of their figures. Finally, on 23 December 2011, the editors of Science retracted the paper in full:
Science is fully retracting the Report “Detection of an infectious retrovirus, XMRV, in blood cells of patients with chronic fatigue syndrome”. Multiple laboratories, including those of the original authors, have failed to reliably detect xenotropic murine leukemia virus– related virus (XMRV) or other murine leukemia virus (MLV)–related viruses in chronic fatigue syndrome (CFS) patients. In addition, there is evidence of poor quality control in a number of specific experiments in the Report … Given all of these issues, Science has lost confidence in the Report and the validity of its conclusions … We are therefore editorially retracting the Report. We regret the time and resources that the scientific community has devoted to unsuccessful attempts to replicate these results.
Three months later, the Whittemore Peterson Institute fired Judy Mikovits amid concerns over the integrity of her work and her collaboration with an outside scientist, as reported in the multidisciplinary scientific journal Nature:
The scientist behind a study that linked chronic fatigue syndrome to a virus has lost her job and is now facing accusations that she has misrepresented data. Judy Mikovits … was fired on 29 September after she clashed with the institute’s president and co-founder, Annette Whittemore, over the work of another researcher.
The following day, in what seems to be a separate development, a blogger posted a figure from a 2009 paper that Mikovits co-authored in Science alongside one that Mikovits used in a recent presentation. The two figures, which are used to describe different results, look identical, except for the labeling.
A few months after that, Mikovits was arrested in southern California “on an ‘out of county warrant’ from Washoe County, Nevada, for allegedly taking lab notebooks, a computer, and other material from the Whittemore Peterson Institute in Reno, Nevada, after the WPI fired her.” The arrest came in conjunction with a lawsuit from WPI that sought a restraining order to block Mikovits’ destruction of data which they maintained belonged to the institute:
After Mikovits was terminated on 29 September, she wrongfully removed laboratory notebooks and kept other proprietary information on her laptop and in flash drives and in a personal e-mail account. WPI, a nonprofit organization that’s based on the campus of the University of Nevada, Reno, also won a temporary restraining order that forbids Mikovits from “destroying, deleting, or altering” any of the related files or data.
The charges were dropped, not because of the merits of the case, but due to a variety of complicating legal factors related to the family that runs the Whittemore Peterson Institute:
On 11 June, the district attorney’s office for Washoe County filed a petition to dismiss the criminal charges against Mikovits without prejudice (which means they can file a related complaint in the future), a clerk to the Justice Court of Reno told ScienceInsider.
Mikovits, who was briefly jailed on the charges, is still defending herself in the civil case, which has taken several bizarre twists, including a judge who had ruled against Mikovits recusing himself. The judge removed himself from the case because he received campaign donations from WPI co-founder Harvey Whittemore, who himself has been criminally charged with making illegal campaign contributions to a federal official …
Assistant District Attorney John Helzer, who filed the dismissal, says Whittemore’s legal troubles factored into his decision. “There’s a lot going on with the federal government and different levels that wasn’t occurring when we first became involved with prosecuting this case,” says Helzer. “And we have witness issues that have arisen.”
ParticipantBill7, here’s a listing of underlying health conditions and other recognized risk factors for Covid-19 patients, which the CDC posted last month:
Diabetes mellitus.
Chronic lung disease, including
asthma
chronic obstructive pulmonary disease (COPD)
emphysema.
Cardiovascular disease.
Immunocompromised condition.
Chronic renal disease.
Pregnancy.
Neurologic disorder, neurodevelopmental, intellectual disability, including
dementia, memory loss, or Alzheimer’s disease
seizure disorder
Parkinson’s disease
migraine/headache
stroke
autism
aneurysm
multiple sclerosis
neuropathy
hereditary spastic paraplegia
myasthenia gravis
intracranial hemorrhage
altered mental status.
Chronic liver disease.
Other chronic disease, including
hypertension
thyroid disease
gastrointestinal disorder
hyperlipidemia
cancer or history of cancer
rheumatologic disorder
hematologic disorder
obesity
arthritis, nonrheumatoid
musculoskeletal disorder other than arthritis
mental health condition
urologic disorder
cerebrovascular disease
obstructive sleep apnea
fibromyalgia
gynecologic disorder
embolism, pulmonary or venous
ophthalmic disorder
hypertriglyceridemia
endocrine
substance abuse disorder
dermatologic disorder
genetic disorder.
Former smoker.
Current smoker.Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019 — United States, February 12–March 28, 2020
https://www.cdc.gov/mmwr/volumes/69/wr/mm6913e2.htmParticipantBy the way, I saw a list of “comorbidities” for COVID-19 patients, and the list included conditions such as a history of migraine headaches, having a skin cancer lesion removed in the past, and others which don’t seem very relevant to the viral infection.
ParticipantNYT: ‘Nearly All Patients Hospitalized With Covid-19 Had Chronic Health Issues, Study Finds’
Yes, that’s an interesting study. The most common comorbidities were hypertension (56.6%), obesity (41.7%), and diabetes (33.8%)…
Yet, to put these numbers into perspective, they should be compared to the prevalence of these conditions in the general population of the US.
The leading comorbidity is hypertension, affecting 56.6% of the patients. For the overall adult population of the US, the prevalence of hypertension (high blood pressure) is estimated to be about 45% [HHS]. Not a huge difference in those numbers.
Next up is obesity, affecting 41.7% of the patients. For comparison, what percentage of the US population is obese? “The prevalence of obesity was 42.4% in 2017~2018″ [CDC data]. So it’s about the same percentage.
Next up is diabetes, affecting 33.8% of the patients. Among the US population overall, 10.5% of the population is estimated to have diabetes [CDC, 2018]. So diabetes appears to be a more significant risk factor for being hospitalized with a COVID-19 infection.
More to the point, how does this data actually support the “anti-lockdown” position? It somehow doesn’t matter as much if people afflicted with diabetes or asthma, for example, get sick and die from the coronavirus?
ParticipantBoogaloo, here’s some additional information about Hydroxychloroquine vs. Chloroquine.
This journal article recommends HCQ (hydroxychloroquine) instead of CQ (chloroquine), for reasons including fewer side effects and safety during pregnancy.COVID-19: a recommendation to examine the effect of hydroxychloroquine in preventing infection and progression
Dan Zhou, Sheng-Ming Dai, Qiang Tong
Journal of Antimicrobial Chemotherapy, Published: 20 March 2020
https://academic.oup.com/jac/advance-article/doi/10.1093/jac/dkaa114/5810487Gastrointestinal responses, such as vomiting and diarrhoea, are the most common adverse effects of these two drugs. Patients with long-term exposure to CQ suffer from severe side effects, such as retinopathy, circular defects (or bull’s eye maculopathy), diametric defects in the retina and cardiomyopathy. Elderly patients and usage beyond dosage limits are also associated with toxicities of CQ therapy. In contrast, HCQ has a lower level of tissue accumulation, which may explain the fact that it is associated with fewer adverse events than CQ, but still potentially influences the prevention and treatment of malaria to a similar level. Indeed, only high-dose and long-term (over 5 years) intake of HCQ is likely to contribute to the development of retinopathy, which is in agreement with the current preference of HCQ use in therapy. While CQ exerts a number of severe side effects on fetal development, HCQ is strongly recommended for pregnant patients with an autoimmune disease as it prevents the development of congenital heart block due to a potential inhibitory effect of type I interferon production. The outbreak of SARS-CoV-2 has placed many pregnant women at high risk of infection (several infected cases have been reported); HCQ, rather than CQ, should be considered as a potential therapeutic solution for these patients, given its safety profile in pregnancy. More importantly, the maximum tolerable dose for HCQ is 1200 mg, which has an antiviral effect equivalent to 750 mg CQ (for which the maximum tolerable dose is 500 mg). This indicates that HCQ can be administered at a higher dosage and may therefore achieve a more powerful antiviral effect.
ParticipantNo surprises in this recent study, despite all the warnings about hydroxychloroquine “possibly increasing the risk of Torsade de pointes (TdP) and sudden cardiac death”.
“In the largest reported cohort of COVID-19 patients [201 of them] to date treated with chloroquine/hydroxychloroquine {plus minus} azithromycin, no instances of TdP or arrhythmogenic death were reported.”
The Effect of Chloroquine, Hydroxychloroquine and Azithromycin on the Corrected QT Interval in Patients with SARS-CoV-2 Infection
https://www.ahajournals.org/doi/abs/10.1161/CIRCEP.120.008662Participant“12.3% of New York state has tested positive for novel coronavirus antibodies”
The report actually indicates that in 7 regions of NY state (out of a total of 11 regions), the percentage testing positive is only 3% or less.
A regional breakdown of the results is below:
Region, Percent Positive
Capital District 2.2%
Central NY 1.9%
Finger Lakes 2.6%
Hudson Valley (Without Westchester/Rockland) 3%
Long Island 11.4%
Mohawk Valley 2.7%
North Country 1.2%
NYC 19.9%
Southern Tier 2.4%
Westchester/Rockland 13.8%
Western NY 6%Amid the ongoing COVID-19 pandemic, Governor Andrew M. Cuomo today announced the results of the state’s completed antibody testing study, showing 12.3 percent of the population have COVID-19 antibodies. The survey developed a baseline infection rate by testing 15,000 people at grocery stores and community centers across the state over the past two weeks.
ParticipantLatest data for England and Wales show deaths from all causes are significantly higher than the 5-year average, and deaths attributed to COVID-19 are significantly higher than the 5-year average number of deaths from influenza and pneumonia.
Influenza and pneumonia deaths (unrelated to COVID-19) continue to be about the same as the 5-year average. This is important, because it shows that the deaths attributed to COVID-19 weren’t boosted by adding all the influenza and pneumonia deaths into the COVID-19 numbers.
There was no double-counting in this analysis, the graphs show deaths from either COVID-19 or “Influenza and Pneumonia”.
“A death can be registered with both COVID-19 and Influenza and Pneumonia mentioned on the death certificate. Because pneumonia may be a consequence of COVID-19, deaths where both were mentioned have been counted [in this analysis] only in the COVID-19 category.”
<a
https://www.ons.gov.uk/visualisations/dvc807/fig1/line/index.htmlParticipantA tale of two cities, Seattle and New York City:
“The initial coronavirus outbreaks in New York City emerged at roughly the same time as those in Seattle. But the cities’ experiences with the disease have markedly differed… There are many explanations for this divergence. New York is denser than Seattle and relies more heavily on public transportation, which forces commuters into close contact… New York also has more poverty and inequality than Seattle, and more international travellers… ”
“It’s also true, however, that the cities’ leaders acted and communicated very differently in the early stages of the pandemic. Seattle’s leaders moved fast to persuade people to stay home and follow the scientists’ advice; New York’s leaders, despite having a highly esteemed public-health department, moved more slowly, offered more muddied messages, and let politicians’ voices dominate…”
“In early March, as [King County Executive] Dow Constantine was asking Microsoft to close its offices and putting scientists in front of news cameras, de Blasio and New York’s governor, Andrew Cuomo, were giving speeches that deëmphasized the risks of the pandemic, even as the city was announcing its first official cases. De Blasio initially voiced caution, saying that “no one should take the coronavirus situation lightly,” but soon told residents to keep helping the city’s economy. “Go on with your lives + get out on the town despite Coronavirus,” he tweeted on March 2nd—one day after the first covid-19 diagnosis in New York. He urged people to see a movie at Lincoln Center.”
“On the day that Seattle schools closed, de Blasio said at a press conference that “if you are not sick, if you are not in the vulnerable category, you should be going about your life.” Cuomo, meanwhile, had told reporters that “we should relax.” He said that most infected people would recover with few problems, adding, “We don’t even think it’s going to be as bad as it was in other countries.”
ParticipantNot so sure about Sweden’s approach. Sweden’s numbers looks bad compared to its neighbors on either side (Finland and Norway).
Sweden does the least testing, but still has the most cases, per million population.
The deaths in Sweden (per million population) are much greater (about six times greater) than in Norway or Finland.Cases per million population
Finland 826
Norway 1,383
Sweden 1,846Deaths per million population
Finland 34
Norway 37
Sweden 217Tests per million population
Finland 14,493
Norway 28,614
Sweden 9,357[data from Worldometer]
ParticipantWHO: No Evidence COVID-19 Antibodies Protect From Potential Re-Infection
From that same article (linked above),
“As the hunt for a vaccine continues around the world, the WHO has formed an international alliance to ensure that treatments are distributed fairly. French President Emmanuel Macron, European Commission President Ursula von der Leyen and the Bill and Melinda Gates Foundation are involved in the alliance.”But,
Scientists fear the hunt for a coronavirus vaccine will fail and we will all have to live with the ‘constant threat’ of COVID-19“The first question we do not know is ‘do you get natural immunity to this disease if you have had it, for a prolonged period of time?'” Whitty said. “Now if we don’t then it doesn’t make a vaccine impossible but it makes it much less likely and we simply don’t know yet.
ParticipantRegarding Dr D’s warnings about inflation resulting if something like “Medicare for All” was set up in the USA, I’d like to point out…
“Today, the United States spends more than $3.2 trillion a year on health care… At $10,000 per person, the United States spends far more on health care per capita and as a percentage of GDP than any other country on earth in both the public and private sectors while still leaving 28 million Americans uninsured and millions more under-insured.” [according to Bernie Sanders]
So if these large amounts of money are already being spent, how can making the system more efficient (cutting out the insurance company middleman profits and negotiating drug prices down) be necessarily inflationary?
ParticipantHuskynut: “And here’s another great article comparing the responses of various countries to analyse the most effective responses:”
https://medium.com/@tomaspueyo/coronavirus-learning-how-to-dance-b8420170203eThat’s an impressive article. As the author Tomas Pueyo puts it, we need to “relax the harsh social distancing measures in a careful way to avoid a second outbreak.“
I mention this here because “a second outbreak” could give another peak, potentially higher than the first one (whenever that happens to be reached). It seems fairly obvious that the actual peak is not independent of the interventions, since more interventions can result in an earlier peak, and removal of all interventions could result in a new peak, higher than what was previously thought to be the peak.
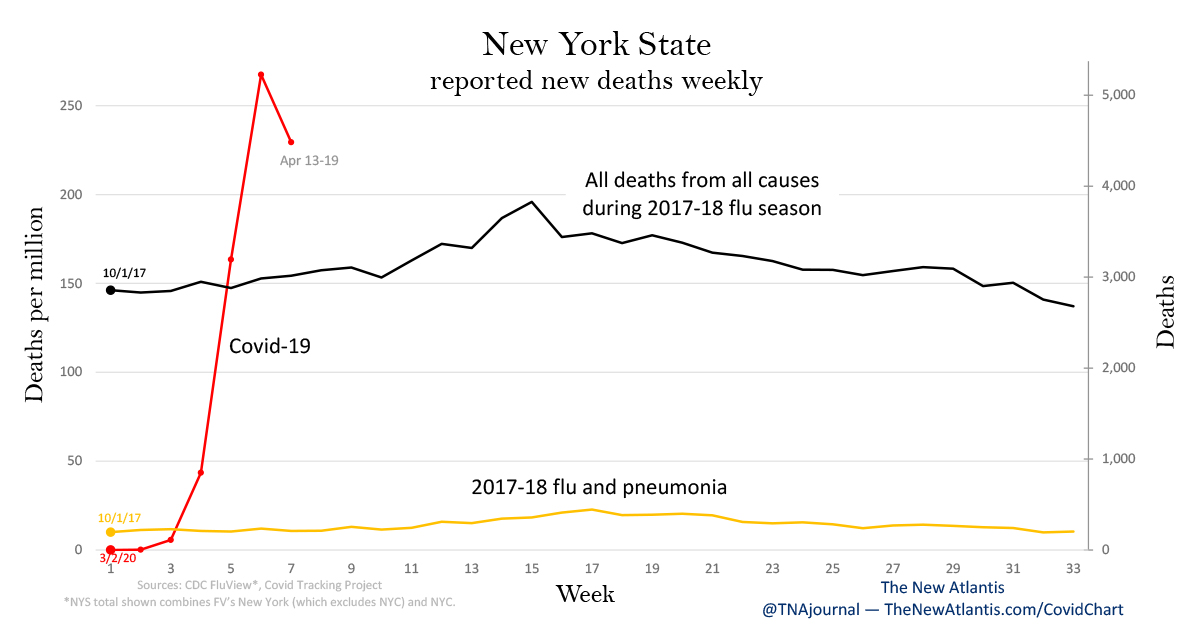
ParticipantThis graph for New York State :
 Participant
ParticipantThe updated graph from The New Atlantis:
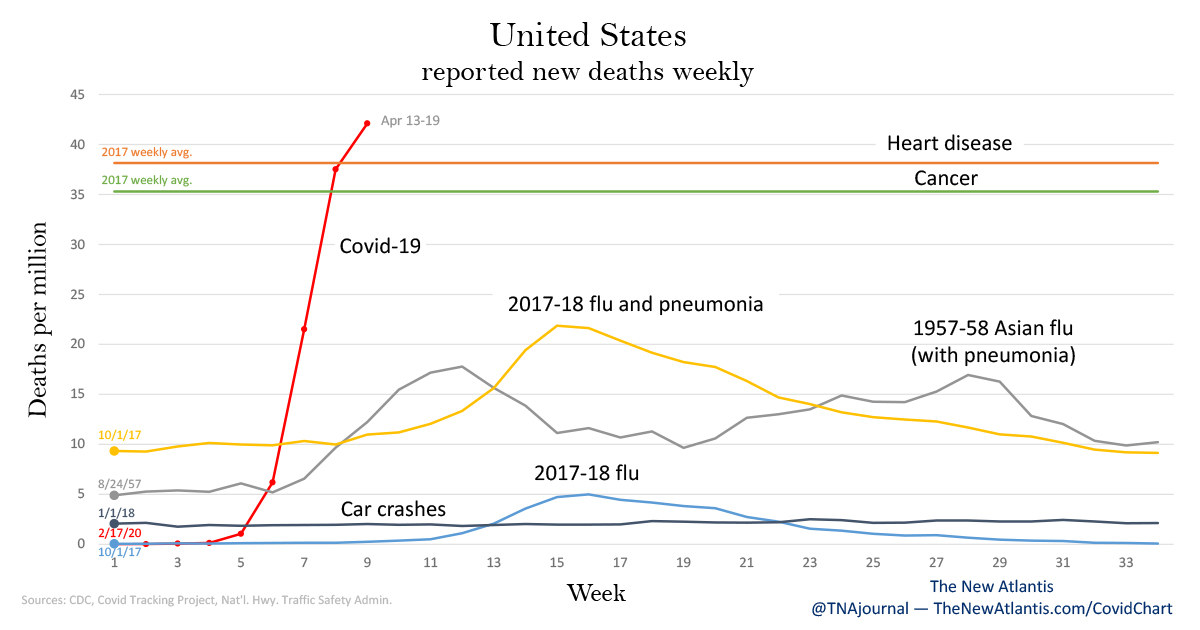
https://www.thenewatlantis.com/publications/not-like-the-flu-not-like-car-crashes-not-like#updates
ParticipantNew York City is apparently “ahead of the curve.”
The cases, hospitalizations, and deaths all seem to have peaked more than a week ago.(see the Daily Counts graph, linked below)
https://www1.nyc.gov/site/doh/covid/covid-19-data.pageParticipantI appreciated Martenson’s critique of the Stanford study. Seems like there’s too much attempted persuasion out there, in various forms, without the backing of actual facts and knowledge.
ParticipantToday’s artwork made me think of this:
 Participant
Participant“Fun Fact” and some implications:
The SARS-CoV-2 virus persists in fecal samples for an average of 27 days, which is 10 days longer than its persistence in respiratory tract samples. A separate preliminary examination of environmental contamination of hospital room air, equipment, personal objects, and toilets at the University of Nebraska Medical Center found widespread contamination even among low-acuity patients without active cough. These research results have grave implications for household protection measures upon discharge for children not yet toilet trained and for parent education, home infection protocols, and postepidemic school preparedness.
From the aforementioned study on ICU beds for children:
https://journals.lww.com/jphmp/Abstract/publishahead/COVID_19_in_Children_in_the_United_States_.99293.aspxParticipant• US Coronavirus Study Warns Sick Children Could Overwhelm Health System
Back in December, the UK was already facing a shortage of paediatric intensive care (PICU) beds, following “an increase in severe breathing problems in children driven by winter viruses and infections, including flu… many of whom are on a ventilator to help them breathe.”
‘Breaking point’: fears over lack of intensive care beds for children
Exclusive: critically ill children rushed to units across England as NHS struggles to find bedsCritically ill children are being rushed from one part of England to another because NHS hospitals are running short of intensive care beds in which to treat them, the Guardian can reveal.
An increase in severe breathing problems in children driven by winter viruses and infections, including flu, means some are having to be transferred sometimes many miles from their home area because there are not enough paediatric intensive care (PICU) beds locally.
Specialist doctors who staff the units say the situation is “dangerous and rotten for the families” involved and that staff are firefighting to handle the number of children needing sometimes life-saving care, many of whom are on a ventilator to help them breathe.
-
AuthorPosts