Omicron is the best vaccine available. You can pick between BA.1 and BA.2. That allows us to do a little overview, also because “new“ findings have come out recently. New only in the sense that the media now report on them for the first time, not because we didn’t already know.
Then again, how would YOU know, if not through Joe Rogan, and his recent guests Dr. Malone and Dr. Mc Cullough, and websites like Peak Prosperity and the Automatic Earth? Media capture has been pretty total for 2 years, because 1/ bad news sells better than good news, and 2/ Big Pharma owns the discussion, through its ownership of media and medical “experts”.
That’s all about to change. Omicron can -and will- still be sold as a potentially devastating disease, but if the numbers don’t add up, people will stop listening and reading. So the media’s hands will be forced. The treatment of Joe Rogan is only the culmination of that, of so many voices since early 2020, and it’s good it led to him.
Because Joe doesn’t care, he’s bigger than all of the media assembling against him, and he did nothing but give some people a voice and a space that were being ostracized -and still are, maybe even more-, and Spotify is a Sweden-based company, which not many will be able to touch.
Yeah, yeah, Neil Young, Joni, Streisand, they’re all in Biden and Pelosi’s age-range, but do you think many people will care who are not over 70, if and when Omicron keeps on lowering death numbers? Or are they more likely to side with Canadian truckers and their ideas of freedom?
Will Justin send the army to “take care” of the protests? You would almost hope so. I don’t think he’s stupid enough, not even him, but he’s in an ugly spot. All he would have had to do is go talk to them, but then that’s the overriding theme here, isn’t it, to not talk, let alone discuss?
The idea has been all along to NOT talk to Dr. Malone and Dr. Mc Cullough, or Joe Rogan, or anyone else who doesn’t toe the Pfizer line. And at some point, like when people realize Omicron is the best vaccine available, all that’s left is to enforce mandates with police or armed forces. As I said, you’d almost hope they do it. The “let them eat cake” moment.
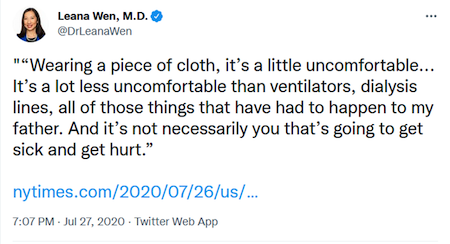
I saw this pic yesterday of a headline from German TV channel NTV, which says Pfizer will sue Denmark for loosening its vaccine mandate, because fewer people will get jabbed, and that means less profit. How much of this will we see?
Back to reality: We have found (or rather, seen confirmed) in the last 2 weeks or so that:
1/ Masks don’t work. The CDC admitted that the cloth masks they recommended for 2 years have no effect whatsoever. But along their own lines of “evidence”, neither do surgical masks, which have holes 1000x bigger than a virus particle. N95 masks could work to some extent, but only if they’re fitted perfectly, by a professional, every time they’re worn.
Maybe the fact that the US government, and CDC and FDA, waited 2 years in promoting them tells you the whole story. And yes, P100 masks might work to some extent, but at that point we might as well go for full-blown gas-masks. In short, face masks “for Covid” have been as entirely useless as they have been completely destructive, in the lives of all of us, but in particular our children.
But the masks still haven’t been as big a disaster as:
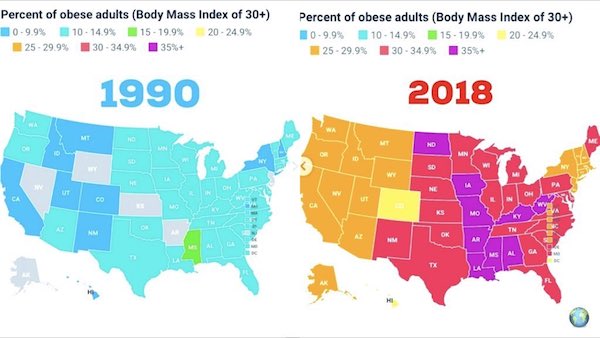
2/ Lockdowns don’t work. For 2 years running, all the media and their loyal followers have been citing the CDC, FDA and Johns Hopkins University. But now that Johns Hopkins releases a report that says lockdowns prevented only 0.2% of potential deaths, crickets are a very popular life form all of a sudden. What’s not to love? But yeah, we get it, good news doesn’t sell. In the same vein, an “imminent” Russian invasion of Ukraine, tanks in the streets of Kyiv, gets a lot more clickbait than “nah, all quiet on the eastern front”.
But the lockdowns haven’t been as big a disaster as (we’re working up to a climax here):
3/ The vaccines don’t work.
3.1/ The vaccines were never needed.
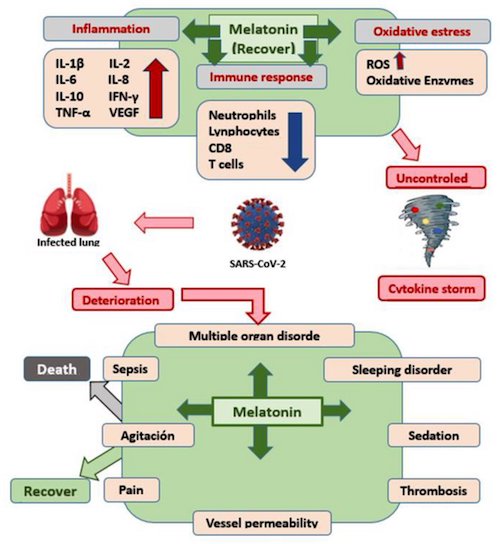
The way to create demand for them was to prohibit all other substances that could have saved millions of lives in prophylaxis or early treatment. As I’ve said repeatedly, I think vitamin D could have prevented 50% of all infections and deaths, zinc could have taken care of the next 25%, and for the remaining quarter an entire scala of repurposed drugs, ivermectin, HCQ, fluvoxamine, melatonin, aspirin etc. would have been enough.
You don’t have to aim for zero. Bring the numbers down by 50-75-90%, and any reason to lock down or wear masks is gone. Pfizer needed to ban all these substances, and ban the possible news coverage of their potential, to get an EUA for its vaccine. And that’s why they were all swept under the carpet. Thing is, there are millions of dead bodies under that carpet, too.
But not only were they never needed:
3.2/ The vaccines don’t work.
To be honest: what we know in early February 2022 is that yes, they do seem to “work” for a few months, we’re not exactly sure how or how long. That should never be a question about a vaccine, however, and if it is, call it something else. Moreover, as far as they “work”, they do that by -trying to- take over control from your immune system, which you cannot survive without. Your best option today is to have an immune system strong enough to fight off the vaccine, which is as insane as it sounds. A booster 3rd or 4th or 12th shot will work for even less time, and in the meantime you run the risk of spike proteins lingering and gathering in all of your organs, including your heart and brain. For the rest of your life.
Because:
3.3/ The vaccines cause enormous damage.
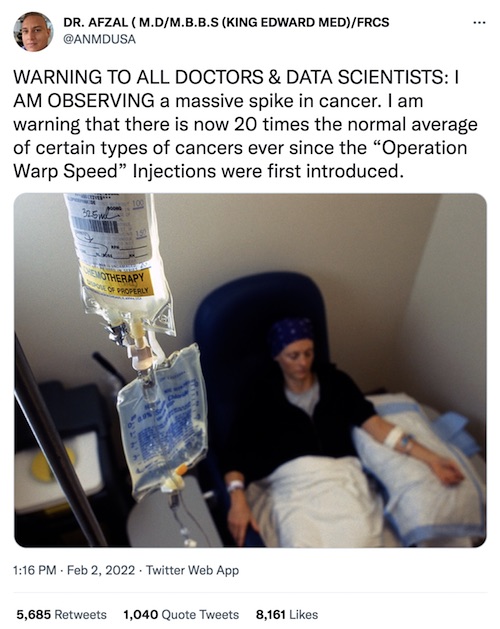
The main issue about mRNA vaccines is not even the scores of vaxxed young athletes dropping dead, or the elevated numbers of 10-15 year olds who have myocarditis, devastating as they are; it’s the long-term consequences, never tested for. I’ve been reading a lot about mRNA and cancer recently. Because I see it pop up all over.
This will not affect everyone. Some of us have robust immune systems. But those that do not, due to age, obesity, you name it, will see the negative effects of spike proteins and other vaccine “by-products”. Not all in the same way, and not all to the same degree. And not all at the same time either. But you’re still all unleashing (cyto-) toxic elements into your body, your bloodstream, your organs.
You’re unleashing more of them with each next shot, or booster, into a body whose immune system has ever less defense against the invading toxic elements. Because your immune system may have “learned” to defend itself against these elements, but then the jabs add ever more of them, and the original antigenic sin kicks in for real. Until the immune system is overwhelmed and gives up.
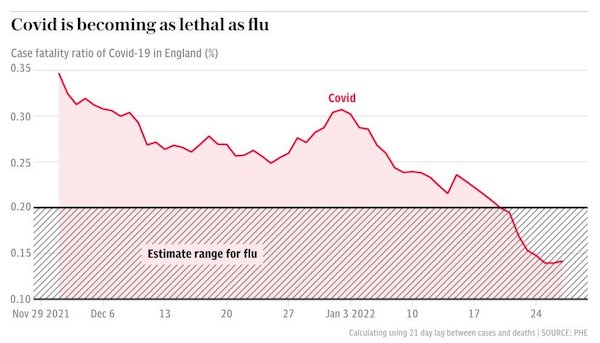
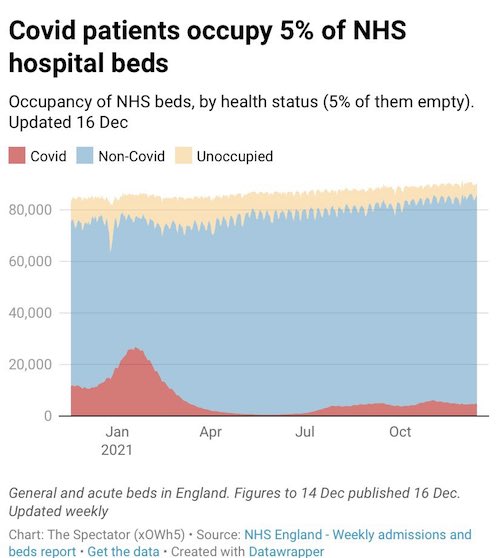
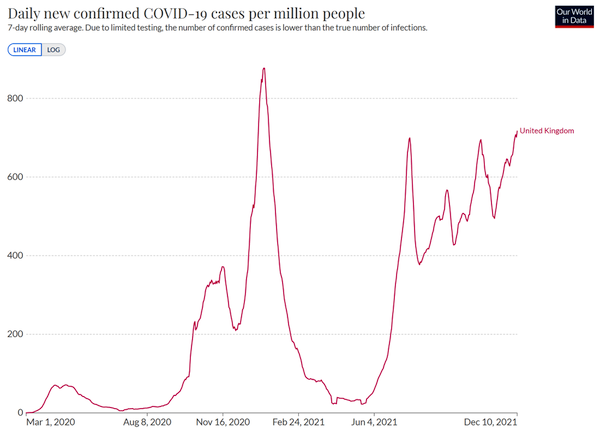
So why the shots, and the boosters? It doesn’t appear to have much to do with logic. In Britain, Covid is already less threatening than the flu. You may argue that this is due to the vaccines, but how realistic is that given we know their efficacy drops so fast you need a booster every few months?
Whereas, if you catch Omicron, and many “Experts” now state that we will all catch it at some point (or more than once), the amount of toxic elements entering your body is manageable. Sure, you may need to boost your immune system, lose weight, change your diet, but how could that ever be a bad thing?
Still, if you combine vitamin D with zinc and perhaps IVM, your chances look much better than with 3-4-5-6 boosters. But, you know, if that’s what you want, go for it. Ditto for face masks, and lockdowns, etc. But with what we know today, there is no reason why anyone should dictate any of these things to you. You’re not any safer because of them.
The main difference appears to be that you, the vaxxed/boosted, have a lot more to be wary about for the rest of your life, 30-40-50 years, from “vaccines” that were poorly tested, and not at all tested for that sort of timespan.
Omicron is a one-off that appears to protect you from all -or most- previous and future Covid variants. The vaccines are geared towards one older variant only, which hardly exists anymore. I won’t advice anyone to get Omicron, but if given the choice between Omicron and Comirnaty, is the choice really that clear?
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Support the Automatic Earth in virustime. Click at the top of the sidebars to donate with Paypal and Patreon.
On Monday, during Sen. Ron Johnson’s five-hour hearing on a “COVID-19: Second Opinion,” Ohio attorney Thomas Renz, who has been representing clients suing the vaccine mandates, presented DOD medical billing data from the Defense Medical Epidemiology Database (DMED) that paints a shockingly disturbing picture of the health of our service members in 2021. According to the military, DMED is the Armed Forces Health Surveillance Branch’s (AFHSB) “web-based tool to remotely query de-identified active component personnel and medical event data contained within the Defense Medical Surveillance System (DMSS).” In other words, it contains every ICD medical billing code for any medical diagnosis in the military submitted for medical insurance billing during any given period of time.
Three military doctors have presented queried data to Renz that shows a shocking and sudden spike in nearly every ICD code for common vaccine injuries in 2021. In a declaration under penalty of perjury that Renz plans to use in federal court, Drs. Samuel Sigoloff, Peter Chambers, and Theresa Long — three military doctors — revealed that there has been a 300% increase in DMED codes registered for miscarriages in the military in 2021 over the five-year average. The five-year average was 1,499 codes for miscarriages per year. During the first 10 months of 2021, it was 4,182. As Renz explained to me in an interview with TheBlaze, these doctors queried the numbers for hundreds of codes from 2016 through 2020 to establish a baseline five-year average. These codes were generally for ailments and injuries that medical literature has established as being potential adverse effects of the vaccines.
Renz told me the numbers tended to be remarkably similar in all those preceding years, including in 2020, which was the first year of the pandemic but before the vaccines were distributed. But then in 2021, the numbers skyrocketed, and the 2021 data doesn’t even include the months of November and December. For example, some public health officials speculate that COVID itself places women at higher risk for miscarriages. But the number of miscarriage codes recorded in 2020 was actually slightly below the five-year average (1,477). However, they were not drastically below the average on any one category in a way that one can suggest it reflects lockdown-related decreases in doctor’s visits, which somehow led to an increase in 2021 diagnoses.
[..] Some other numbers he did not mention at the hearing but gave to me in the interview are the following:
• myocardial infarction –269% increase
• Bell’s palsy – 291% increase
• congenital malformations (for children of military personnel) – 156% increase
• female infertility – 471% increase
• pulmonary embolisms – 467% increase
All these numbers are among the ambulatory visits because those are where the vast number of diagnoses in the military occur. However, Renz did say the increases were indicated in the hospitalized patients as well. I have seen one of the sworn declarations from one of the military doctors, and it states as follows, “It is my professional opinion that the major increases incidences of the above discussed instances of miscarriages, cancers, and disease were due to COVID-19 ‘vaccinations.'”
Two-dose COVID-19 vaccines may after an initial protective window become less effective against symptomatic infection by the Omicron variant than not getting jabbed at all, according to little-noticed findings in a federal study of how well boosters performed against different variants. The “adjusted odds ratio” crossed 1 for vaccinated versus unvaccinated individuals 7-10 months after vaccination, according to the “original investigation” by Atlanta-based CDC researchers, published in the Journal of the American Medical Association last week. That means the vaccinated were more likely than the unvaccinated to have symptomatic Omicron infections beginning at about the time the former become eligible for boosters. When considering the upper bound of the 95% confidence interval, the disparity emerged two months earlier.
Pfizer’s mRNA vaccine performed worse than Moderna’s, the researchers wrote. “The upper bound of the 95% CI was consistently greater than 1 starting at 3 months after second dose” for the former and six months for the latter. By contrast, the odds ratios for either vaccine never got close to 1 for the Delta variant, even for the upper bound. Even as evidence of the short-lived efficacy of the COVID mRNA vaccines continues to mount, federal regulators stepped in Tuesday to block doctors from using monoclonal antibodies to treat COVID patients. The FDA on Monday revoked authorizations for two such treatments against Omicron infections, including the one used by then-President Trump, finding they were “highly unlikely to be active” against the now-dominant variant.
The little-noticed findings in the JAMA study were highlighted by law professor Todd Zywicki, whose natural immunity lawsuit prompted George Mason University to grant him a medical exemption from its vaccine mandate. “Still more confirmation that Pfizer and Moderna’s CEOs know what they are talking about when they state that 2 doses of vax provides insignificant (at best) protection against Omicron,” Zywicki tweeted Tuesday. [..] The adjusted odds ratio of symptomatic Omicron infection for boosted versus unvaccinated individuals was 0.33, and for boosted versus two-dose recipients, 0.34. That means three doses corresponded with an “estimated effectiveness” of 67% over no doses, and 66% over two doses.
The study confirms that “OVERALL vaccine efficacy is zero,” Zywicki told Just the News: The first few months of protection “rapidly approaches zero” around the six-month mark and then goes negative for a few more months. He said the JAMA study was the fourth to find “basically this same negative [vaccine efficacy] effect” that he documented in an Epoch Times op-ed on “original antigenic sin.” Zywicki highlighted research from Toronto, California and Denmark that found negative VE starting two to six months after vaccination. The California study was “slippery,” he claimed, because “the authors appear to have simply arbitrarily set a floor of zero vaccine efficacy.”
The White House said Wednesday that the COVID-19 vaccine regime for kids younger than 4 years old will likely be three doses when it’s approved — and vowed to make millions more hard-to-find Pfizer anti-viral pills available in coming months. Two clinical trials of the Pfizer vaccine on children ages 6 months to 2 years old, and ages 2 to 4 are underway, but the older group hasn’t yet met standards, White House chief medical adviser Dr. Anthony Fauci said at a press conference. “Dose and regimen for children 6 months to 24 months worked well, but it turned out the other group from 24 months to 4 years did not yet reach the level of non-inferiority, so the studies are continued,” Fauci said, referencing effectiveness standard comparison to adults.
“It looks like it will be a three-dose regimen. I don’t think we can predict when we will see it [approved],” he said — adding he can’t speak for the Food and Drug Administration. “We need to be patient,” he said. “That’s why the system works. The FDA is very scrupulous in their ability and in their effort to make sure that, before something gets approved for any age, and especially with children … that they will be safe, and that they will be effective.” Meanwhile, White House officials promised to release millions more Pfizer antiviral pills by June, amid reports that the medicine has been difficult to find in recent weeks. “We’ve purchased 20 million treatment courses of the Pfizer pill and we accelerated delivery of the first 10 million from September to the end of June,” said White House coronavirus response coordinator Jeff Zients.
Unvaccinated Quebecers over 12 years old are now banned from buying groceries at big box stores including Walmart and Costco, while people wishing to access pharmacies inside those outlets will require a store escort. This comes as Quebec’s new vaccine requirement for retail stores over 1500 square meters took effect today. While the new mandate explicitly excluded grocery stores and pharmacies, the Quebec government said they did not consider groceries to be Walmart and Costco’s “principal activity.” The box-store ban comes despite statistics showing that Walmart and Costco are among the top three places where Canadians get their groceries. Quebec’s health minister Christian Dubé is standing by the measure, claiming that the goal is to protect “both the vaccinated and the non-vaccinated.”
An exemption was added for pharmacies located inside big box stores after pharmacy leaders raised concerns in a letter to the government. Unvaccinated people who wish to access those pharmacies must be accompanied by a store employee, who will ensure they make no other purchases. Unvaccinated Quebecers are now subject to the harshest government restrictions in Canada, and some of the strictest in the world. Quebec also requires vaccine passports at government-run liquor and cannabis stores, and a “significant” health tax is on the way. The government also announced that Quebecers would require a third jab for their vaccine passports to remain valid. At one point, the Quebec government even considered banning the unvaccinated from regular grocery stores and pharmacies that offer delivery, but it appears they have abandoned the idea.
While many Americans are beginning to look towards a life after Covid, and some experts are making optimistic predictions about the future of the pandemic, the entire scientific community is not in agreement. Dr Gregory Poland, epidemiologist for the Mayo Clinic and is editor-in-chief of the scientific journals ‘Vaccine’ and one of the nation’s top experts on vaccination and immunology, said this week that the virus could be affecting humans for the next century. In a conversation with MarketWatch on Tuesday he gave a grave prediction that counters what some worldwide global health experts are saying.
Due to the rapid transmission of the Omicron Covid variant combined with its more mild nature, experts are hopeful that it be the strain that transitions the virus from a pandemic to an endemic, meaning the pattern of the virus is stable and predictable. Poland does not share the same optimistic point of view. ‘We are not yet at any stage where we could predict endemicity. We’re not going to eradicate it,’ Poland said. He noted that the virus has shown the ability to infect animals, meaning it can potentially circulate indefinitely as it transmits across species and continues to mutate. Poland believes the virus will circulate for so long that people will still be receiving Covid shots for generations down the line.
‘So let me make a prediction, which will be hard for any of you to hold me to because we will all be dead by then, but your great-great-great-grandchildren will still be getting immunized against coronavirus,’ ‘How can I even say such a thing? If you got your flu vaccine this fall you were immunized against a strain of influenza that showed up in 1918 and caused a pandemic.’ This is not the first grim prediction Poland has made, and he has been correct before. Last month, he told DailyMail.com that he believed 32,000 people would die from Covid between early December to the end of the year. ‘32,000 Americans who think they’re going to be alive to celebrate Christmas and New Years are, no pun intended, dead wrong,’ he said on December 9. ‘Not one of them believes [they will die].’ During that period, 31,000 U.S. Covid deaths were recorded, nearly a spot on prediction, per Our World in Data.
A Florida doctor says families of loved ones hospitalized with COVID-19 are resorting to desperate measures when approved treatments have failed. And when it’s not too late, some have seen tremendous success by sneaking medications prohibited by hospitals to patients, says Eduardo Balbona, an independent internist in Jacksonville. He’s helped dozens of seriously ill patients recover using ivermectin and other drugs and supplements not officially approved in the treatment of COVID-19, he says. Hospitals receive payments from the federal government for treating patients with COVID-19. But those payments are tied to their use of approved treatments only, as outlined in the CARES Act. When there’s nothing left to try under those protocols, families naturally research alternatives, Balbona says, often learning about treatments touted by independent physicians around the country.
Hoping to try anything that might work, families around the country have filed lawsuits asking judges to intervene. In some cases, judges have ordered hospitals to allow the use of other treatments, such as ivermectin. Some of those seriously ill patients have recovered. In other cases, judges have sided with hospitals and declined the families’ requests to try. Meanwhile, independent physicians like Balbona watch helplessly, feeling that when families ask, they should be allowed to try medications they believe can turn critically ill patients around. But independent doctors often have limited hospital privileges and may be banned from seeing their own patients in some hospitals.
The Biden administration is withdrawing its COVID vaccine-or-test mandate for large employers, the U.S. Department of Labor announced today. In pulling the rule, the department said it recognized the Emergency Temporary Standard (ETS) could not be revived after the U.S. Supreme Court blocked it earlier this month. Instead, the Biden administration is working to set a permanent standard for the vaccine mandate based on the Supreme Court’s ruling, according to a notice provided to the court by the Occupational Safety and Health Administration (OSHA). OSHA said in a press release:
“Although OSHA is withdrawing the vaccination and testing ETS as an enforceable emergency temporary standard, the agency is not withdrawing the ETS as a proposed rule. The agency is prioritizing its resources to focus on finalizing a permanent COVID-19 Healthcare Standard.” OSHA could move a version of the vaccine-or-test rule through its rule-making process, but would still likely face legal challenges, according to David Michaels, a former OSHA administrator and professor at George Washington University. The Labor Department’s decision to withdraw the rule means pending legal proceedings will be dropped. The case was on its way back to the 6th Circuit Court of Appeals to be heard on the merits, although the lower court most likely would have followed the Supreme Court’s lead, The New York Times reported.
Without OSHA’s vaccine mandate in effect, employers must follow state and local laws on COVID workplace safety. Some states have banned vaccine mandates for private employees, while other states, like New York, require them. “OSHA continues to strongly encourage the vaccination of workers against the continuing dangers posed by Covid-19 in the workplace,” the Labor Department wrote in the notice of its withdrawal. The Supreme Court on Jan. 13, rejected the Biden administration’s employer mandate. The court’s conservative majority said the administration overstepped its authority by imposing OSHA’s vaccine-or-test rule.
The Food and Drug Administration thought it was appropriate that it be given 75 years to produce data for vaccines, which have proven to be the basis for the biggest public policy disaster in U.S. history. The judge instead ordered it to fork over the documents at a rate over a hundred times faster what it had requested. “I am pleased to report that a federal judge soundly rejected the FDA’s request and ordered the FDA to produce all the data at a clip of 55,000 pages per month!” Aaron Siri, who is the key litigator in the case, announced earlier on his Substack page. But in an update to the legal battle, Siri now indicates that the FDA is dragging its feet while providing flimsy excuses about why it won’t do what it was ordered.
The FDA “has now asked the Court to make the public wait until May for it to start producing 55,000 pages per month and, even then, claims it may not be able to meet this rate,” Siri writes. “The FDA’s excuse?” he asked rhetorically. “As explained in the brief opposing the FDA’s request, the FDA’s defense effectively amounts to claiming that the 11 document reviewers it has already assigned and the 17 additional reviewers being onboarded are only capable of reading at the speed of preschoolers.” Even more ominously for scientific transparency and the rule of law, Pfizer has even intervened in the case. Siri pointed out that the pharmaceutical company’s reps showed up at the recent court trial.
“As the FDA tries to obtain months of delay, guess who just showed upon in the lawsuit? Yep, Pfizer,” he said. “And it is represented by a global chair and team from a law firm with thousands of lawyers. Pfizer’s legal bill will likely be multiple times what it would cost the FDA to simply hire a private document review company to review, redact, and produce the documents at issue. Within weeks, if not days.” “Pfizer is coming in as a third party,” he added. “But Pfizer assures the Court it is here to help expedite production of the documents. Sure it is! Where was Pfizer before the Court ordered the 55,000 pages per month? Right, doing what it normally does: letting the government work on its behalf – like the way the government mandates, promotes, and defends Pfizer’s product.”
“But the government did not please Pfizer this time and so here it comes, likely looking for a second bite at the apple,” Siri said. “Of course the FDA consented to Pfizer appearing.” The federal judge in the case earlier issued a ruling against the FDA that it had to produce 55,000 pages a month, instead of the originally requested 55 years to release all of them. Aaron Siri weighed in on the importance of the court’s ruling. “No person should ever be coerced to engage in an unwanted medical procedure,” Siri said. ”And while it is bad enough the government violated this basic liberty right by mandating the Covid-19 vaccine, the government also wanted to hide the data by waiting to fully produce what it relied upon to license this product until almost every American alive today is dead. That form of governance is destructive to liberty and antithetical to the openness required in a democratic society.”
Appearing on Fox News Tuesday, Senator Rand Paul issued advice on what to do if you find yourself confronted by one of the dwindling numbers of mask wearing “lunatics” who continue to appeal for mass “collectivism”. Host Jesse Watters asked Paul about a recent indecent in which two mask Karens attacked a man for not wearing one, and as he was black, kept yelling ‘Black lives Matter’ at him. “These people clearly aren’t well,” Watters noted, adding “Large swaths of America are in a Covid cult.” The host asked the Senator “As a medical professional, as a genteel Senator and a polite individual, Dr. Rand Paul, what would you recommend Americans do when they are confronted with these mask maniacs, when they are yelled at and screamed at and being recorded on their phone? How should they handle that in a respectful but normal way?”
“See, I would say bear spray but I’m afraid that will get me in trouble so I won’t say that,” Paul jokingly responded. He followed up “I think you should back away and say, ‘Lady, you are crazy, leave me the hell alone,’ but you should not confront her.” Paul continued, “You should not use violence. Back away and just say look, can you not find some other lunatic friends to hang around with?” Paul also noted that “Really this is a difference between individualism and collectivism.” “I have an opinion, but I’m not wanting to enforce it on anybody. I’m not telling you that you can’t wear a mask. I’m just saying don’t make me wear a mask when it doesn’t work,” the Senator urged.
Great conversation between @JesseBWatters and Sen. Rand Paul on mask mania:
"So really there's no strong evidence that masks work … If anything the disease keeps going up when you have mask mandates. The masks really have had no influence on the pandemic." pic.twitter.com/m4fpwydbiW
Spotify has sided with its podcast superstar over Neil Young. The legendary folk singer gave the streaming behemoth an ultimatum earlier this week, saying he refused to allow his music on the same platform as Joe Rogan. The “Heart of Gold” singer accused Rogan and his podcast of spreading false information about COVID-19 vaccines. Spotify reportedly paid more than $100 million deal to be the exclusive home of Rogan’s show. Young, meanwhile, stands to lose 60% of his streaming income from his defiant stance, he said in a statement on his website. “We want all the world’s music and audio content to be available to Spotify users,” a spokesperson for the company told the Wall Street Journal. “With that comes great responsibility in balancing both safety for listeners and freedom for creators.”
Since the start of the pandemic, the spokesman noted, Spotify has removed more than 20,000 COVID-related podcast episodes. Still, Young’s protests were not sufficient for it to drop its lucrative star talker. “We regret Neil’s decision to remove his music from Spotify, but hope to welcome him back soon,” the spokesperson added. Rogan’s podcast has attracted an estimated 11 million listeners. Young’s letter — which is now deleted from his website — did not mince words in accusing the streaming giant of giving an undeserved platform to Rogan and his COVID-19 vaccine “misinformation.” “I want you to let Spotify know immediately TODAY that I want all my music off their platform,” wrote the 76-year-old rock icon. “I am doing this because Spotify is spreading fake information about vaccines – potentially causing death to those who believe the disinformation being spread by them.”
[..] Young thanked his publisher Hipgnosis and his label Warner Records/Reprise for supporting his ultimatum. “Losing 60% of worldwide streaming income by leaving SPOTIFY is a very big deal, a costly move, but worth it for our integrity and beliefs. Misinformation about COVID is over the line.” He went on to nudge other artists to take a similar stance. “I sincerely hope that other artists can make a move, but I can’t really expect that to happen,” Young said. “I did this because I had no choice in my heart. It is who I am. I am not censoring anyone. I am speaking my own truth.”Although Young did not specifically note which episodes he took issue with, Rogan did recently host Dr. Robert Malone, the “anti-vaxxer epidemiologist” who was recently booted from Twitter for alleged dissemination of vaccine misinformation…
Powell: It will soon be appropriate to raise the Federal Funds target rate. …. Reducing our balance sheet will occur after the process of raising interest rates has begun.
Mish: Inflation suggests it was appropriate a year ago. At the very least, expanding the balance sheet now is ridiculous. Yet the Fed will still expand through March 2022. The Fed made similar statements a year or so ago, and thus committed to let inflation burn higher regardless of what happened in the interim.
Powell: Reductions will occur over time in a predictable manner. primarily through adjustments to reinvestments so that securities will roll off our balance sheet. … The Committee has not made decisions regarding specific timing, pace or other details of shrinking the balance sheet. We will discuss these matters in upcoming meetings and provide additional information at the appropriate time.
Mish: This implies a very slow balance sheet reduction. In practice, it’s highly likely the next recession hits before the Fed gets seriously underway with balance sheet reduction.
Chris Rugaber, Associated Press: Are rate hikes at consecutive meetings on the table? Is every meeting a live meeting? Would the Fed consider frontloading rate hikes?
Powell: It is not possible to predict with much confidence what path our policy will take will prove appropriate. … We will be humble and nimble. … We will be led by the incoming data.
Mish: Just like the Fed was led by the incoming inflation data? Here’s the real deal: The Fed will do what it wants and will bend subsequent wishy-washy statements to justify whatever policy it wants to set.
Nick Timiraos, Wall Street Journal: Apart from moving faster to shrink [balance sheet] holdings are there any other ways you and your colleagues are seriously thinking about recalibrating this process? And finally, how much disagreement is there on how you use tools?
Powell: I am afraid to tell you those are all great questions, but those are questions the committee is just turning to now.
Mish: This implies the Fed has been on autopilot all this time, and amazingly is still there despite huge inflation every step of the way. The Fed announced QE through March of 2022 and despite everything that happened, did not waver from announced policy. Yet, the Fed wants us to believe it will decide policy on the basis of incoming data!
The row over Ukraine is the outgrowth of an aggressive US posture toward Russia since the collapse of the Soviet Union three decades ago, driven by hegemonic policymakers and war profiteers in Washington. Understanding that background is key to resolving the current impasse, if the Biden administration can bring itself to alter a dangerous course. Russia’s central demands – binding guarantees to halt the eastward expansion of NATO, particularly in Ukraine, and to prevent offensive weapons from being stationed near its borders – have been publicly dismissed by the U.S government as non-starters. In rejecting Russian concerns, the Biden administration claims that it is upholding “governing principles of international peace and security.”
These principles, Secretary of State Anthony Blinken says, “reject the right of one country to change the borders of another by force; to dictate to another the policies it pursues or the choices it makes, including with whom to associate; or to exert a sphere of influence that would subjugate sovereign neighbors to its will.” The US government’s real-world commitment to these principles is non-existent. For decades, the US has provided critical diplomatic and military cover for Israel’s de-facto annexations, which have expanded its borders to three different strips of occupied territory (the West Bank, Gaza, and Syria’s Golan Heights). The US is by far the world leader in dictating policies to other countries, be it who their leaders should be; how little to pay minimum-wage workers; or how to share energy supplies.
The Biden administration continues to subjugate sovereign countries to its will, whether it’s “neighbors” like blockade-targeted Cuba; coup-targeted Venezuela; sanctions-targeted Nicaragua; or far-away countries like US military-occupied and sanctions-targeted Syria. Biden just recently embraced the longstanding Monroe Doctrine of a US sphere of influence by declaring Latin America to be the United States’ “front yard.” When not making sanctimonious public pronouncements, US officials are quietly able to acknowledge the real principles that guide their actions. According to the Washington Post, one US official specializing in Russia “believes the Russians are still interested in a real dialogue.” Russia’s real aim, this official says, is “to see whether Washington is willing to discuss any sort of commitment that constrains U.S. power.”
The official added: “The Russians are waiting to see what we’re going to offer, and they’re going to take it back and decide is this serious. Is this something we [the Russians] can sell as a major victory for security, or is it just, from their point of view, another attempt to fob us off and not give us anything?”
In my first article of the year, I must thank everyone who has followed us, and read us, and commented, especially those of you who have made donations both to the Automatic Earth, and to the Monastiraki kitchen for the homeless in Athens, Greece. Both don’t reach millions of people, but the thousands we do connect with, we reach them well. Every reader who learns something is a win, and every homeless person who gets a good meal, well, that’s obvious.
Thank you so much. You are the ones who make this happen.
If I say that 2020 was the year of the virus, and 2021 the year of the vaccine, most people would probably agree. But 2021 was so much more than that; it was also the year of propaganda, media capture and narrative control at levels beyond anything we’ve ever seen. Even if many -most- people haven’t experienced it that way.
And that has likely had more negative impact on us than the vaccine itself. A close call perhaps, I know. The good thing that has come out of this is that so much of it has been exposed. Much of the underlying tendencies towards authoritarianism, and disregard for truth, and blind desire for profit, for a Great Reset, population control, abandonment of freedoms and human rights, it’s all there now for us to see.
We need to act upon that exposure. Get rid of Fauci, Walensky, Pfizer, CDC, and their peers across the planet, of the WHO, of all health “experts” that receive income from/via Pfizer et al (which is the vast majority), put a halt to the influence of money (Bill Gates) on health policy. A society, a country, need to be their own boss over their own fundamental policies. And that means paying for it ourselves.
And not have policies easily changed by a group of politicians and unelected officials (“experts”) who happen to have grabbed power at a particular point in time. A society needs roots, and ours have been uprooted. From principles, from laws, from rights. This will not be easy, we already gave them a 2 year advantage, but if we don’t use this time when the spotlights are directed at them, we will lose even much more than we have already lost. We’ve let them play their games, virtually uncontested, and we cannot afford that.
This appears to culminate in Twitter’s handling of Joe Rogan and Robert Malone recently, and that’s fine, Twitter is not big enough to tackle Rogan, while CNN and MSNBC audiences are drops in the ocean compared to Joe’s. They bit off one too big for them to chew.
But that’s just the US, and that’s just one podcaster, one voice. The control virus that has come with the corona virus has delved much deeper into the world’s various societies. Just yesterday, we saw video from my country of birth, Holland, where police set attack dogs on peaceful elderly protesters, and say what you will, but that country is neither free nor a democracy. That claim is 100% obsolete.
That it is accepted regardless gives credence, and a lot, to Matthias Desmet and his “Mass Formation Syndrome” theories, but we should not really need his analysis, useful as it may be, to figure out what is going on. All we need to do is take a step back and wonder what the hell is going on. To ponder how we saw our societies 2+ years ago, how we ourselves would have seen these recent developments in the light of back then. We can’t have forgotten all of it?!
That Anthony Fauci is still in his job is absolutely insane. He became head of the US National Institute of Allergy and Infectious Diseases (NIAID), 40 years ago, he’s 81, older than Joe Biden. He’s been building ties to Big Pharma, especially Pfizer, all that time, in the shadows, the best place for such deals.
He was in his position when Pfizer received the biggest criminal fine in US corporate history in 2012, of $2.3 billion, for lying and cheating and more. Now, a few years later, Fauci works with Pfizer and the rest of Big Pharma, and makes their owners billionaires and their shareholders very rich. He is the very last person who should have been in his where he is, both 2 years ago and now.
Fauci is not the best doctor in the US, he’s just the best connected to the pharma industry. That guarantees Americans the worst deal they could get, not the best. And of course anyone else at the upper echelons of the NIAID, CDC, FDA, they need to go too. Fauci et al put them there.
In the US and elsewhere, any politician, individual or through their party or otherwise, and any health experts, individual or through their organization or company, who have received funds from Big Pharma or Bill Gates, should be discarded, put out by the curb. We should be able to figure this out, because it’s NOW that they stand exposed. Perhaps not TO Covid, but certainly BY Covid.
It’s the only way we can cleanse the system. Which is needed if we want to survive, with our health, our conscience, and our freedoms and rights. We have let an enormous amount of mold, rot, grow at the pillars of our societies, and we should be glad we can see it now, because this allows us to exterminate it.
We cannot allow Pfizer to gain even more influence over our health systems. Which will be a very hard fight, because our politicians and experts handed them $100s of billions, which they are using as we speak to buy more politicians and lobbyists and influence, and profit.
You can’t stop this by voting for another party. Pfizer probably has more lobbyists on K Street than all of Big Oil put together. And they have them in party and every every country that matters, in every strategic position that matters, and they will soon have many more. No, you must cut their entire voice out of the politics and health care of your society. Yes, very difficult, sure. But today, you can at least see them. For a short time. That won’t last.
Along with all that the World Economic Forum, and their Great Reset, it will have to go. They don’t do anyone any good but themselves. A big club that we ain’t in. Which reminds me:
The Automatic Earth has shifted a lot towards Covid over the past 2 years, and surely many readers are not 100% happy with that. But the financial world is still captive to central banks that won’t allow price discovery, which makes “markets” just fake pantomimes that former investors get rich in while the poor suffer.
While the climate issue has been captured by the likes of COP 26, a toy for the rich who want to make you pay to “go green”, in accordance with Davos and the WEF. I feel sorry for the well-meaning people who expect anything from that set-up. Nobody who owes their money or their power to fossil fuels will voluntarily give up either, but they will make you fork over for windmills and solar cells whose energy dynamics you don’t actually understand.
Just like with Covid, if you want to free yourselves from the narrative, you will have to open your eyes and go to battle. An untested vaccine won’t set you free, and neither will an electric car. Those two are just things you are being sold by the narrative.
But believe you me, the no. 1 issue today is the vaccines. We need to stop those, before all of our children grow up with timebombs in their bodies. Every jab means more spike proteins, and boosters are worse because they come after your immune system has learned, and prepared for, how to attack those proteins, who by then may be in every organ in your body. And attack them it will, because they are toxic agents.
I don’t want to tell people to get a vaccine or not, but I do want to tell them to be very careful, to get informed well, and only then give their consent, if they decide to get jabbed. It’s just that you have to be confident that your immune system is strong enough to defend you from the effects of the vaccine, and that’s the opposite of what 99% of people understand is happening to them.
So, 2020 year of the virus, 2021 year of the vaccine, and 2022 year of the adverse effects of the vaccines?! And/or a grand awakening?
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Support the Automatic Earth in virustime. Donate with Paypal, Bitcoin and Patreon.
Clown World
https://twitter.com/i/status/1475657029150986241
cloth masks
.@DrLeanaWen: "Don't wear a cloth mask. Cloth masks are little more than facial decorations. There's no place for them in light of Omicron." pic.twitter.com/Kpoj18sxdi
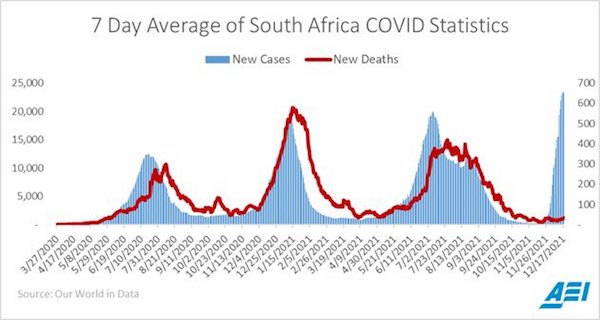
The rapid spread of the Omicron variant of COVID-19 worldwide “may have positive implications in terms of decreasing the Covid-19 burden of severe disease,” according to a new study funded by the Gates Foundation and South African, U.S. and U.K. government agencies. Led by researchers in South Africa, where the variant was first identified, it’s the latest study to suggest the pandemic is approaching endemic status, calling into question the benefits of strict mitigation policies beyond high-risk groups. The preprint, not yet peer-reviewed, found that the “neutralizing immunity” provided by Omicron infection extended to the Delta variant, which appears to be more “pathogenic” than Omicron and still comprises a substantial proportion of COVID infections in several countries.
It was based on 15 participants, mostly vaccinated, who were tested at a median of four days after symptom onset and again 14 days later. They showed 14.4-fold increased neutralization of subsequent Omicron infection but also 4.4-fold increased neutralization of Delta infection, as determined by antibody response. Two of the original 15 were later excluded because they did not “detectably neutralize Omicron at either timepoint.” The results suggest Omicron infection “may result in decreased ability of Delta to re-infect those individuals,” the researchers wrote. If the new variant is indeed less severe, “the infection may shift to become less disruptive to individuals and society.”
Beyond South African institutions, the 30-odd researchers in the study are affiliated with Columbia University, the University of Washington and Imperial College London. The enhanced immunity to Delta was “especially” strong for vaccinated participants, tweeted lead author Alex Sigal, who is affiliated with the Africa Health Research Institute, University of KwaZulu-Natal and Germany’s Max Planck Institute for Infection Biology.
While it is now evident that Omicron is rapidly replacing Delta, due to a combination of increased transmissibility and immune escape, it is less clear how the severity of Omicron compares to Delta. In Ontario, we sought to examine hospitalization and death associated with Omicron, as compared to matched cases infected with Delta. We conducted a matched cohort study, considering time to hospitalization or death as the outcome, and analyzed with a Cox proportional hazards model. Cases were matched on age, gender, and onset date, while vaccine doses received and time since vaccination were included as adjustment variables.
We identified 6,314 Omicron cases that met eligibility criteria, of which 6,312 could be matched with at least one Delta case (N=8,875) based on age, gender, and onset date. There were 21 (0.3%) hospitalizations and 0 (0%) deaths among matched Omicron cases, compared to 116 (2.2%) hospitalizations and 7 (0.3%) deaths among matched Delta cases. The adjusted risk of hospitalization or death was 54% lower (HR=0.46, 95%CI: 0.27, 0.77) among Omicron cases compared to Delta cases. While severity may be reduced, the absolute number of hospitalizations and impact on the healthcare system could still be significant due to the increased transmissibility of Omicron.
The SARS-CoV-2 Omicron variant has multiple Spike (S) protein mutations that contribute to escape from the neutralizing antibody responses, and reducing vaccine protection from infection. The extent to which other components of the adaptive response such as T cells may still target Omicron and contribute to protection from severe outcomes is unknown. We assessed the ability of T cells to react with Omicron spike in participants who were vaccinated with Ad26.CoV2.S or BNT162b2, and in unvaccinated convalescent COVID-19 patients (n = 70). We found that 70-80% of the CD4 and CD8 T cell response to spike was maintained across study groups.
Moreover, the magnitude of Omicron cross-reactive T cells was similar to that of the Beta and Delta variants, despite Omicron harbouring considerably more mutations. Additionally, in Omicron-infected hospitalized patients (n = 19), there were comparable T cell responses to ancestral spike, nucleocapsid and membrane proteins to those found in patients hospitalized in previous waves dominated by the ancestral, Beta or Delta variants (n = 49). These results demonstrate that despite Omicron’s extensive mutations and reduced susceptibility to neutralizing antibodies, the majority of T cell response, induced by vaccination or natural infection, cross-recognises the variant. Well-preserved T cell immunity to Omicron is likely to contribute to protection from severe COVID-19, supporting early clinical observations from South Africa.
Dr. Anthony Fauci said Wednesday it’s “conceivable” that a fourth dose of a COVID-19 vaccine will be recommended to protect against the Omicron variant — though more research is needed about how well the current boosters prevent severe disease. “Before we start talking about a fourth shot, it would be very important for us to determine the durability of protection, particularly against severe disease for the third-shot booster of an mRNA [vaccine] and the second shot of a [Johnson & Johnson],” Fauci said at a White House COVID-19 task force press briefing. But Fauci said it’s possible that more protection will be necessary against the variant.
“It is conceivable that in the future, we might need an additional shot, but right now, we are hoping that we will get a greater degree of durability of protection from that booster shot,” Fauci said. “So we’re going to take one step at a time, get the data from the third boost and then make decisions based on scientific data.” Fauci warned that Omicron has been better at evading the immunity provided by vaccines, causing breakthrough infections. But he said that “boosters bring back up that degree of protection to a level that is approximately what it was before.” “So boosters are critical in getting our approach to Omicron to be optimal,” he said.
Australians may have to receive two or even three Covid jabs each year to maintain defences against the virus if early results on the efficacy of booster shots turn out to be a useful guide. Weekly data published just before Christmas by the UK’s Health Security Agency shows the effectiveness of both the Pfizer and Moderna boosters against symptomatic diseases is lower for the Omicron than the Delta variant across all periods after the injection. The analysis included 147,597 Delta and 68,489 Omicron cases in the UK. The agency stressed the “results should be interpreted with caution due to the low counts and the possible biases related to the populations with highest exposure to Omicron (including travellers and their close contacts) which cannot fully be accounted for”.
The UK data showed both Pfizer and Moderna boosters had 90% effectiveness against symptomatic diseases from the Delta variant up to at least nine weeks. By contrast, efficacy against the Omicron strain was about 30% lower, and appeared to drop away further after nine weeks. Israel has already begun administering a second booster dose to follow the original three-dose treatment, and at least one US medical centre is considering recommending staff have a second booster. Medical experts in Australia said results beyond the 12-week dataset would be needed to get a longer term picture. Jaya Dantas, a professor of international health at Curtin University, said it was still early days for the understanding of the efficacy of the vaccinations but “it appears that there might be a need for regular boosters”. “You might need boosters, say maybe two a year or three a year,” Dantas said, with elderly people more likely to be in line for a triple annual dose.
The Centers for Disease Control (CDC) is finally withdrawing the PCR test for COVID for it is seriously flawed and is incapable of distinguishing between the COVID and influenza viruses. I have stated that I was tested 5 times in 2020 and all were negative only to have two doctors, including the head of pulmonary at the hospital, inform me that they believed I had COVID despite the tests because they were “invalid” and that was back then. Social Media was blocking any discussion about that calling it conspiracy theory and misinformation. This agenda to terrorize the public for political gain has been at the heart of the abuse of politics and media intruding into the medical field. Doctors who have gone along with this terror campaign are a disgrace to their field.
The CDC is withdrawing the COVID PCR Test and the media is not making this front page. The withdraw of the COVID PCR test as valid for detecting and identifying SARS-CoV-2 is critical for all the restrictions and lockdowns. It appears that the collapse in the approval ratings for BIDEN has sent a shock wave through the Democrats as they see their own demise on the horizon. They are now back-peddling in hopes of surviving the 2022 elections. The CDC has stated on its website: “After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only.”
The CDC has finally admitted that the PCR test cannot even differentiate between SARS-CoV-2 and influenza viruses. As I was told personally that the test was invalid, the politics in the USA realizes that this is not going well and they need to shift gears or all be thrown out in the next election.
The newly updated CDC guidelines don’t require testing at the end of isolation because PCR tests can stay positive for up to 12 weeks, CDC Director Dr. Rochelle Walensky told “Good Morning America” Wednesday. “So we would have people in isolation for a very long time if we were relying on PCRs,” Walensky said. Walensky also addressed Tuesday’s news from the FDA that, according to early data, rapid antigen tests may be less sensitive when it comes to the omicron variant.
“We do know that the most sensitive test you can do is a PCR test,” Walensky said. “So if you have symptoms and you have a negative antigen test, we do ask you to go and get a PCR to make sure those symptoms are not attributable to COVID.” Walensky said rapid tests do work “quite well,” especially in places where people are being tested regularly, like at schools. “They may not work as well as they have for the delta variant,” Walensky said, but “we still are encouraging their use.”
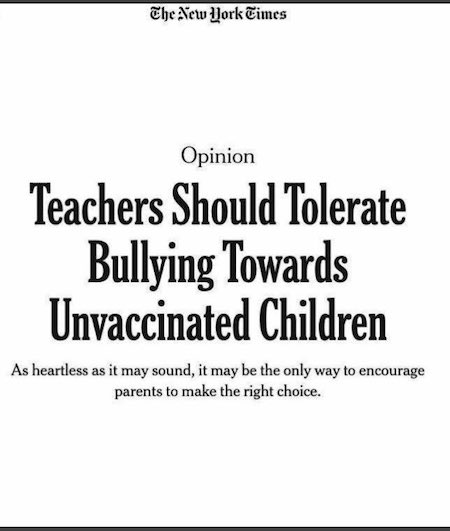
Tolerate
CDC Director Walensky on the reduction of quarantine: “It really had a lot to do with what we thought people would be able to tolerate.”
This says it all. As much tyranny as the people will tolerate. This ends when we demand they end it—unconditionally.pic.twitter.com/63aodHJMut
“Over a half million followers gone in a blink of an eye..”
I think maybe Malone got banned because he’s about to go on Joe Rogan. Whose interview with Peter McCullough was the most popular one he did at 40 million listeners.
A social media purge may be accelerating against reporting and commentary perceived at odds with conventional storylines on COVID-19. Twitter permanently suspended mRNA vaccine pioneer-turned-critic Robert Malone’s account Wednesday for “spreading misleading and potentially harmful information” about the novel coronavirus, according to a notice Malone shared with Just the News. [..] Malone’s only previous sanction was a 12-hour suspension for “posting something with a commercial intent (near as I could tell),” Malone said. He has also received complaints about his tweets required by “German law” over the past year. But he suspects his “big sin” was sharing the Canadian Covid Care Alliance’s analysis of Pfizer’s “adverse event reports” from the first six months of its COVID vaccine’s emergency use authorization.
In a Substack essay Wednesday, posted before his account went down, Malone characterized that analysis as showing the “inoculations cause more illness than they prevent” – a claim at odds with mainstream scientific opinion. France-owned newswire service AFP countered the Canadian Covid Care Alliance’s claims several months ago and similar claims earlier this month, arguing the Pfizer data had been misconstrued. It quoted a Pfizer spokesperson who said the causes of the 1,223 fatalities among 158,893 adverse effects had not been verified, and reflect “spontaneous” reports from sources in several countries. An FDA spokesperson said “the vast majority of the deaths reported are not directly attributable to the vaccines.”[..]
The last archive of Malone’s Twitter page Wednesday afternoon doesn’t show him promoting the analysis. But his final tweets linked to a British Medical Journal investigation into “data integrity issues in Pfizer’s vaccine trial” and a related interview. He also claimed the World Economic Forum had published a “roadmap” for “managing us,” citing WEF’s “Transformation Map” on peace and resilience. “This is the face of global information control and warfare,” he told Just the News, referring to the map. “It’s not just Twitter.” Malone announced his suspension on Substack and encouraged readers to sign up for his newsletter. “Over a half million followers gone in a blink of an eye,” he wrote, referring to his Twitter audience. “That means I must have been on the mark, so to speak.”
Created less than a month ago to share “deeper” essays and research, the newsletter had 35,000 subscribers Wednesday morning, he told Just the News. It “just exploded” after Twitter deplatformed him later in the day. A much larger audience will get to hear from Malone soon. He’s scheduled to go on Joe Rogan’s podcast, by some measures the most popular in America.
Watch this video of the Pfizer 6 month data which shows that Pfizer’s COVID-19 inoculations cause more illness than they prevent. Plus, an overview of the Pfizer trial flaws in both design and execution.
Joe Rogan’s sold out Vancouver show, scheduled for April 20, has been canceled after the podcast host said he likely would be unable to enter Canada from the U.S., where he lives, because he is not vaccinated against COVID-19. In a Dec. 24 episode of his podcast, “The Joe Rogan Experience,” Rogan told his guest, comedian Tim Dillon, that Rogan’s springtime show in Vancouver was likely to be canceled because of COVID-19 restrictions in British Columbia. The Canadian territory requires proof of vaccination to gain entry into some indoor businesses and event spaces, including Rogers Arena, where Rogan’s show was set to take place.
“I should probably say this because I haven’t yet. My 4/20 show that’s sold out in Vancouver — I don’t think that’s happening,” Rogan said. “I don’t think I can even get into the country. I’m not vaccinated. I’m not gonna get vaccinated. I have antibodies, it doesn’t make any sense.” Rogan announced in an Instagram post in early September that he had been diagnosed with COVID-19 after running a high fever and said he had been taking a mix of medications, including monoclonal antibody treatments, Z-Pak, the anti-inflammatory drug prednisone and the antiparasitic ivermectin, which the FDA has said is not recommended for treating COVID-19.
“It is outrageous and unfair that a story that is completely accurate and points out an important legal distinction between the two versions of vaccines gets blocked and my account suspended..”
Twitter suspended the account of Just the News founder John Solomon for sharing an article about the legal distinctions between Pfizer’s fully approved and emergency use authorization (EUA) COVID-19 vaccines, which could affect the legality of vaccine mandates. The social media company is also warning users who click the link to the article from individual tweets that it “may be unsafe” and “could lead to real-world harm.” An immunologist who reviewed the article told Just the News he saw nothing wrong with it factually. Solomon’s Dec. 27 tweet shared the link and headline: “Pfizer to continue distributing version of COVID-19 vaccine not fully approved by FDA.”
The report noted that Pfizer and several experts have claimed that the fully approved Comirnaty vaccine has the same ingredients and manufacturing process as the EUA vaccine, known as Pfizer-BioNTech. But it also cited the FDA’s acknowledgment that the two are “legally distinct” owing to more stringent requirements for the Comirnaty vaccine, whose biologics license application (BLA) was approved. In a legal challenge to the U.S. military’s vaccine mandate, a federal judge ruled in November that “FDA licensure does not retroactively apply to [EUA vaccine] vials shipped before BLA approval.” U.S. District Judge Allen Winsor cited DOD guidance that limits mandates to fully approved vaccines, which must be “produced at approved facilities.”
“It is outrageous and unfair that a story that is completely accurate and points out an important legal distinction between the two versions of vaccines gets blocked and my account suspended,” Solomon told Just the News. “The distinction was important enough for a federal judge to note. The story and my post weren’t unsafe,” he said. “The only threat is to the safety of the 1st Amendment afflicted by Twitter’s wrongheaded decision.” [..] According to the notice Solomon received, Twitter “temporarily limited” his account features for 12 hours because the tweet violates its policy on “spreading misleading and potentially harmful information” related to COVID.
Is Pfizer refusing to make the fully authorized version available, while continuing to sell an EUA product because doing so could open up Pfizer and BioNTech to legal liability issues? Pfizer and an HHS spokesperson talked to The Washington Post in a previous “fact check,” and claimed that there’s no additional legal immunity benefits between the EUA product and Comirnaty. However, these entities have never explained why Pfizer and the federal government would go through the trouble of recognizing two legally distinct products. An EUA fully protects the drugmaker and grants zero legal recourse to the patient. This surefire protection measure was bolstered by the PREP act and other measures implemented to shield COVID companies from liability. Now, here’s where it all gets very nefarious.
Due to a law passed during the Reagan Administration, in order for drug makers to be granted more robust legal liability protection for their vaccines, they must first secure full approval for the children’s version of their shot. Steve Kirsch has explained this at length last month on his Substack. Additionally, Robert Kennedy Jr mentioned it on a recent podcast with Mikhaila Peterson. I looked into these claims extensively, and they appear accurate. The National Childhood Vaccine Injury Act (NCVIA), which was passed into law in 1986, provides a legal liability shield to drug manufacturers if they receive full authorization for all ages. Is Pfizer seeking approval for children so that it can protect itself from lawsuits? The company is working with regulators, even clandestinely altering vaccine ingredients (a process that should require them to get full approval for an entirely separate product), in a seeming bid to clear the path to legal indemnity.
Surely, there’s also a monetary incentive in play, but maybe there’s another reason why Pfizer, Moderna, and others are working relentlessly to authorize their products for children, who face near-zero risk from COVID-19, but continue to showcase alarming side effects from the vaccine. A vaccine on the children’s schedule provides a definitive, government-incentivized liability boost. If Comirnaty becomes available for all ages, that means Pfizer receives an extensive, additional layer of protection. Is Big Pharma using children as legal human shields for their products?
RFK: If a vaccine is introduced under EUA, the maker can’t be sued. When it IS approved, they can be sued. Unless they can get it recommended for children. That’s why 5 year olds are being jabbed.
RFK Jr On Vaccines Liability: "They Know This Is Going To Kill And Injure A Huge Number Of Children, But They Need To Do It For The Liability Protection" pic.twitter.com/CL62aAIv14
Florida Surgeon General Joseph Ladapo accused the Biden administration of “actively preventing the effective distribution of monoclonal antibody treatments” in the United States, according to a Tuesday letter addressed to Secretary of Health and Human Services Xavier Becerra.The Biden administration recently paused shipments of COVID-19 antibody treatments manufactured by major drug companies Regeneron and Eli Lilly amid claims that such treatments are not effective against the omicron variant of the coronavirus. The federal government continues to supply Sotrovimab, a monoclonal antibody from the company Glaxosmithkline, which reportedly does work against omicron. Ladapo concluded his letter by referencing comments Biden made Monday that there wasn’t a solution by the federal government to end the nearly two-year-old pandemic.
“There is no federal solution. This gets solved at the state level,” Biden said at the time in response to Arkansas Republican Gov. Asa Hutchinson warning the president against letting “federal solutions stand in the way of state solutions.” A spokesperson for the Department of Health and Human Services (HHS) pushed back against Ladapo’s assertion, telling Fox News Digital in a statement: “The federal government has and will continue to supply Florida with treatments that can help improve patient outcomes, reduce stress on healthcare facilities, and save lives. We have never stopped allocating or shipping COVID-19 therapeutics to Florida. “With regard to monoclonal antibody treatments, the federal government has allocated about 22,000 doses in just the past two weeks (11,050 doses last week and 10,576 doses this week). That’s in addition to the approximately 28,000 doses of product that they have on hand from their previous orders,” the statement continued.
The true identity of Bitcoin creator Satoshi Nakamoto, who has been one of the financial world’s enduring mysteries, is still unknown. However, Elon Musk says he might have the answer. Musk says hyper-secretive cryptocurrency expert Nick Szabo might be the creator of the world’s most popular cryptocurrency. “You can look at the evolution of ideas before the launch of Bitcoin and see who wrote about those ideas,” Musk told artificial-intelligence researcher Lex Fridman in a podcast on Tuesday. The Tesla CEO also denied the allegations that he could be Satoshi, stating he would not hide it if he were. Musk said while he “obviously” doesn’t know exactly who created Bitcoin, Szabo’s theories seem fundamental to the creation of the world’s leading cryptocurrency.
“It seems as though Nick Szabo is probably, more than anyone else, responsible for the evolution of those ideas,” he said. “He claims not to be Nakamoto, but I’m not sure that’s neither here nor there. But he seems to be the one more responsible for the ideas behind Bitcoin than anyone else. In 2014, a team of researchers studied Nakamoto’s Bitcoin whitepaper alongside the writing of Szabo and 10 other potential creators. “The number of linguistic similarities between Szabo’s writing and the Bitcoin whitepaper is uncanny,” they said, adding that “none of the other possible authors were anywhere near as good of a match.” Before Bitcoin debuted in 2008, Szabo was seen commenting on his blog about his “intent to create a living version of the hypothetical currency.” He had developed a digital money mechanism known as Szabo Bit Gold between 1998 and 2005.
If America’s so free and fair, why is Julian Assange, innocent in natural law, so terrified of being extradited to the USA? And why must journalist Glenn Greenwald live abroad, after heroically helping whistleblower Edward Snowden, now safely ensconced in Russia? American heroes living abroad for fear of the American Security State? Time perhaps to shut up about China? In 2010, Snowden had shared internal NSA documents with Mr. Greenwald, the guardian of American freedoms at the British Guardian newspaper. Facilitated by Greenwald, Snowden divulged that the National Security Agency boasted of having “direct access to the systems of Google, Facebook, Apple, Yahoo, PalTalk, YouTube in 2010; Skype and AOL, and other servers.”
It transpired that, contrary to what you’d been told by officials under oath, “the world’s largest surveillance organization” can and does “obtain targeted communications without having to request them from the service providers and without having to obtain individual court orders.” This is contrary to the Bill of Rights, and the Fourth Amendment to the Constitution, in particular, which specifies that “warrants shall issue” only “upon probable cause, supported by oath or affirmation, and particularly describing the place to be searched, and the persons or things to be seized.” The federal authorities routinely collect data on phone calls Americans make, regardless of whether they have any bearing on a counterterrorism investigation. Tellingly, the tools of Big Media and Big Government had not apprised you of these facts.
It took Snowden to come forth, in his words, “to reveal the criminality.” In Snowden’s poignant words, “You can’t wait around for someone else to act. I had been looking for leaders, but I realized that leadership is about being the first to act. … I’m neither traitor nor hero. I’m an American,” he summed-up so simply. “Thank you for your service,” Mr. Snowden. For his part, a decade before he was broken, an insouciant Assange told the New Yorker that “a social movement to expose secrets could bring down many administrations that rely on concealing reality — including the US administration.” A naïve Assange had vowed to skewer “lying, corrupt and murderous leadership from Bahrain to Brazil.”
With its many epic “data dumps,” Assange’s WikiLeaks enlightened and educated, providing definitive proof that the mass media are lapdogs, not watchdogs. Democratic lapdogs. The colluding quislings of the major American networks and newspapers had actively worked to elect Mrs. Clinton. Thanks to WikiLeaks, Americans also learned of the contempt with which these Democrats hold them. [..] Well, America has jurisdiction over Assange because it has simply asserted it based on trumped-up charges equating his journalism with espionage. Which is why Assange now fears being “Epsteined.”
— Jordan Schachtel @ dossier.substack.com (@JordanSchachtel) December 20, 2021
The autoimmunity issue comes to the foreground.
Sucharit Bhakdi, MD and Arne Burkhardt, MD. [..] a written summary of Dr. Bhakdi’s and Dr. Burkhardt’s presentations at the Doctors for COVID Ethics symposium that was live-streamed by UKColumn on December 10th, 2021.
Why the vaccines cannot protect against infection A fundamental mistake underlying the development of the COVID-19 vaccines was to neglect the functional distinction between the two major categories of antibodies which the body produces in order to protect itself from pathogenic microbes. The first category (secretory IgA) is produced by immune cells (lymphocytes) which are located directly underneath the mucous membranes that line the respiratory and intestinal tract. The antibodies produced by these lymphocytes are secreted through and to the surface of the mucous membranes. These antibodies are thus on site to meet air-borne viruses, and they may be able to prevent viral binding and infection of the cells.
The second category of antibodies (IgG and circulating IgA) occur in the bloodstream. These antibodies protect the internal organs of the body from infectious agents that try to spread via the bloodstream. Vaccines that are injected into the muscle – i.e., the interior of the body – will only induce IgG and circulating IgA, not secretory IgA. Such antibodies cannot and will not effectively protect the mucous membranes from infection by SARS-CoV-2. Thus, the currently observed “breakthrough infections” among vaccinated individuals merely confirm the fundamental design flaws of the vaccines. Measurements of antibodies in the blood can never yield any information on the true status of immunity against infection of the respiratory tract. The inability of vaccine-induced antibodies to prevent coronavirus infections has been reported in recent scientific publications.
The vaccines can trigger self-destruction A natural infection with SARS-CoV-2 (coronavirus) will in most individuals remain localized to the respiratory tract. In contrast, the vaccines cause cells deep inside our body to express the viral spike protein, which they were never meant to do by nature. Any cell which expresses this foreign antigen will come under attack by the immune system, which will involve both IgG antibodies and cytotoxic T-lymphocytes. This may occur in any organ. We are seeing now that the heart is affected in many young people, leading to myocarditis or even sudden cardiac arrest and death. How and why such tragedies might causally be linked to vaccination has remained a matter of conjecture because scientific evidence has been lacking. This situation has now been rectified.
[..] Conclusion Histopathologic analysis show clear evidence of vaccine-induced autoimmune-like pathology in multiple organs. That myriad adverse events deriving from such auto-attack processes must be expected to very frequently occur in all individuals, particularly following booster injections, is self-evident. Beyond any doubt, injection of gene-based COVID-19 vaccines places lives under threat of illness and death. We note that both mRNA and vector-based vaccines are represented among these cases, as are all four major manufacturers.
"There is no vaccine that you put into your muscle that can ever protect you against an infection of the respiratory tract… anyone who says otherwise is either ignorant or he's lying."
Pathogenic priming, as originally described, is the act of exposing people (or animals) to epitopes that match human proteins, leading to the inducement of autoreactogenic antibodies that attack tissues anywhere in the body. I described pathogenic priming in April, 2020 and predicted that tissues across the body could become afflicted due to exposure to COVID-19 proteins. Evidence is mounting that points to pathogenic priming contributing morbidity and mortality among the vaccinated, including • Increased all-cause mortality • Histopathological evidence of autoimmunity across various organs. An important message, with data, came to me today on one of my many email threads. I am sharing this on Popular Rationalism with permission Ronald Kostoff, who fowarded the analysis below.
[..] Commenting on the above, Ronald wrote: “If the autopsy findings are confirmed by other pathologists with additional samples, and if they are combined with the findings of Dr. Hoffe (>60% inoculant recipients have elevated D-dimer tests and evidence of clotting) and Dr. Cole (increase in cancers after inoculation, including twenty-fold increase in uterine cancer), we are seeing a disaster of unimaginable proportions. The conclusion (if supported by further data) is that essentially EVERY inoculant recipient suffers damage, with more damage after each shot. The damage could be cumulative, and the shots may be synergistic. Given the seriousness of the types of damage (autoimmune diseases, cancer, re-emergent dormant infections, clotting/strokes, cardiac damage, etc.), these effects will translate into lifespan reduction, which should be counted as deaths from the inoculations.
So, in the USA, where ~200M people have been fully inoculated, the number of deaths will not be the 10,000 or so reported in VAERS, or 500,000-1,000,000 scaled-up deaths from VAERS, but could be closer to tens of millions (or more) when the inoculation effects play out! What the above three findings (Burkhart, Hoffe, Cole, and I suspect many others who have not yet come forward) show is that the post-inoculation effects are not rare events (as reported by the media-gov’t), but are in actuality frequent events. They may be, in fact, universal, with different degrees of severity and damage for each recipient. The question is whether it is possible to reverse these inoculation-based adverse events.
Can the innate immune system be fully restored? Can the microclotting be reversed? Can the autoimmunity be reversed? There is a wide spectrum of opinions on whether this is possible, none of which is overly convincing. Are we headed for the situation where the ~30% unvaxxed will be devoting their lives to operating whatever is left of the economic infrastructure and serving as caretakers for the vaxxed? The above sounds extreme, and maybe when more data are gathered from myriad credible sources the results and conclusions may change, but right now the above data seem to synchronize with the demonstrated underlying mechanisms of damage. Additionally, we seem to be doubling down on inoculations, with fourth booster being proposed for Israel, and UK suggesting quarterly boosters.”
Facebook wrote that my predictions of an ever-evolving virus, pressured by an ever-expanding population-level immune pressure caused by mass vaccination are wrong. I have always said that mass vaccination would cause more infectious variants to expand in prevalence and become dominant. Making it impossible for mass vaccination fanatics to ‘stay ahead of the virus’ as they always claim. The consecutive dominance of alpha, beta, gamma, delta and, more recently, the omicron variant is merely proof that my predictions have come true.
Even though the highly infectious Omicron does not seem to be highly virulent, there can be no doubt that continued mass vaccination campaigns that will soon use updated boosters against Omicron are at high risk of provoking ADE (antibody-dependent enhancement of disease) and will thereby dramatically enhance the incidence of severe disease in vaccinees. I have explained this in my most recent video message to the WHO, urging them not to allow vaccination against Omicron. (Second call to WHO: Please, don’t vaccinate against Omicron) Damania’s comments on my scientific analysis and predictions have already been proven void.
Furthermore, arguments he’s been trying to tease out from experts, like Paul Offit, have been seamlessly refuted in my interview with Del Bigtree (Geert Vanden Bossche Warns of Covid-19 Vaccination Catastrophe). Damania obviously has a big mouth, but has never been responsive to engaging in an open scientific debate, while being heavily paid to spout misinformation and misinterpretations on the evolutionary dynamics of this pandemic. Of which he clearly doesn’t understand due to his limited knowledge of virology, immunology and vaccinology. “Separating the wheat from the chaff” (Some guidance to separating the wheat from the chaff) is, therefore, a ‘must read’ for all those who are trying to find credible information enabling them to make informed decisions about their own health and that of their children. In that regard, cheap and hollow one-liners like those uttered by Damania are clearly not very helpful.
Israel has begun administering a fourth Covid-19 vaccine dose to triple-vaccinated test subjects. The Jewish state is already planning on offering an extra booster shot to the elderly and vulnerable. 150 medical workers at the Sheba Medical Center near Tel Aviv began receiving a fourth dose of Pfizer’s Covid-19 vaccine on Monday. These workers have all received three doses – an initial two plus a booster – already, and will be monitored for six months as researchers assess their antibody levels and monitor for potential side effects, CBS News reported. “Hopefully, we’ll be able to show here … that this fourth booster really provides protection against the Omicron,” Jacob Lavee, a professor at the prestigious hospital, told the Associated Press.
The trial is believed to be the first test of a fourth booster dose anywhere in the world, and comes at a time when the Omicron variant is rapidly becoming the dominant coronavirus strain worldwide. Although the new variant typically causes only mild to moderate symptoms in those it infects, it is believed to be highly transmissible, and studies have shown vaccines to be significantly less effective against it when compared to earlier variants. Israel was the first country on earth to vaccinate a majority of its citizens, and was one of the first countries in which the vaccines were shown to lose efficacy over time. Since then, the country has been an early trailblazer in administering booster shots, and around 45% of the Israeli population has received a third dose of the Pfizer shot.
Massie
The booster shot was never about reducing symptoms.
The booster shot was about trying to maintain the lie that the vaccine could prevent people from contracting and spreading COVID.
That lie was the basis for all vaccine mandates, and it completely disintegrated this month.
The Food and Drug Administration (FDA) recently authorized two antiviral pills, one from Pfizer and one from Merck, making them the first at-home treatment for COVID-19 that has been touted as a game changer in the fight against the pandemic. However, experts told NBC News that the pills will require careful monitoring by doctors and pharmacists. While Pfizer’s Paxlovid has been authorized for use in children 12 and over with underlying health conditions including heart disease or diabetes, a component of the antiviral cocktail could have serious and life- threatening interactions with drugs including blood thinners, statins and depressants, NBC reported.
“Some of these potential interactions are not trivial, and some pairings have to be avoided altogether,” Peter Anderson, a professor of pharmaceutical sciences at the University of Colorado told NBC News. “Some are probably easily managed. But some we’re going to have to be very careful about,” he added. In a statement to The Hill, a Pfizer spokesperson said, “The potential for drug-drug interactions (DDI) for Paxlovid was examined in a series of in vitro studies, as well as clinical DDI studies.” The spokesperson further elaborated on the antiviral pill and said that Paxlovid is comprised of the active protease inhibitor Nirmatrelvir, as well as a low-dose of 100 mg of Ritonavir.
“Its effect on drug metabolism may result in drug interactions, and some drugs may be contra-indicated. However, in light of the fact that Paxlovid has a short duration of treatment of five days, combined with a low dose of Ritonavir of 100 milligrams, we believe that healthcare professionals should find most DDIs to be generally manageable,” the statement reads. “The product’s emergency use authorization fact sheets include information on drug interactions and contraindications. Healthcare providers should consider the potential for drug interactions prior to and during PAXLOVID therapy and review concomitant medications during PAXLOVID therapy,” the spokesperson added.
“We think that the documentation basis is really, really flimsy. We are afraid that we will have to use a remedy that is ineffective at best and, at worst, jeopardises people’s treatment..”
Denmark has recently become the first EU country to approve a new COVID-19 treatment by the US pharmaceutical company Merck, but the decision has run into difficulties as the country’s general practitioners refuse to prescribe the treatment due to insufficient knowledge of how it works, calling it ineffective and potentially even harmful. The Danish Society for General Practice (DSAM), which is the professional community of general practitioners, has criticised the National Board of Health for its recommendations concerning COVID-19 treatment. Earlier, the Danish Health and Medicines Authority has approved the US drugmaker Merck’s anti-COVID pill molnupiravir, which also goes by the name Lagevrio, to treat at-risk patients with symptoms, making Denmark the first EU country to do so. So far, 50,000 pills have been purchased.
Explaining their reluctance to administer it, DSAM’s COVID-19 spokesman Anders Beich cited the drug’s poor documentation. “We think that the documentation basis is really, really flimsy. We are afraid that we will have to use a remedy that is ineffective at best and, at worst, jeopardises people’s treatment,” he told Danish Radio. According to him, patients may receive proper treatment too late. “There is a tendency to believe that once you have received your treatment, you will do well. It may be that both doctor and patient think that now the patient is in treatment. But if the treatment is ineffective, then you will waste time, and there is a risk that the disease will get worse without action being taken,” Beich mused.
The same criticism was echoed by Danish Medicines Agency, an independent council that makes recommendations to the regions on the use of various drugs. “We already have treatments that work for the group of patients where the pill is intended for use. Treatments that work much better and are documented much better than this pill,” chairman Steen Werner Hansen said. “So in the worst case, this would prevent some patients from getting a relevant treatment,” he concluded.
Justification and Objectives: the serious health, social and economic consequences of COVID-19 have forced an urgent search for preventive methods, such as vaccines, among others, and therapeutic methods that could be alternatives to the drugs currently used. In this sense, it must be accepted that one of the most recommended has been the administration of melatonin. The present study proposes to carry out a systematic review of its possible role in the treatment and/or prevention of COVID-19.
Material and methods: a systematic review of the literature related to the prevention of COVID-19 through the administration of melatonin was carried out, following the sequence proposed by the Prisma Declaration regarding the identification and selection of documents, using the specialized health databases Trip Medical Database, Cochrane Library, PubMed, Medline Plus, BVS, Cuiden and generic databases such as Dialnet, Web of Science and Google Scholar for their retrieval. Appropriate inclusion and exclusion criteria are described for the articles assessed. The main limitation of the study has been the scarcity of works and the lack of defining a specific protocol in terms of dosage and administration schedule.
Results: once the selection process was completed, and after an in-depth critical analysis, 197 papers were selected, and 40 of them were finally used. The most relevant results were: (1) melatonin prevents SARS-CoV-2 infection, (2) although much remains to be clarified, at high doses, it seems to have a coadjuvant therapeutic effect in the treatment of SARS-CoV-2 infection and (3) melatonin is effective against SARS-CoV-2 infection.
Discussion: until group immunization is achieved in the population, it seems clear that we must continue to treat patients with SARS-CoV-2 infection, and, in the absence of a specific and effective antiviral therapy, it is advisable to continue researching and providing drugs that demonstrate validity based on the scientific evidence. In this regard, we believe that the available studies recommend the administration of melatonin for its anti-inflammatory, antioxidant, immunomodulatory, sleep-inducing, CD147, Mpro, p65 and MMP9 protein suppressing, nephrotoxicity-reducing and highly effective and safe effects.
Conclusions: (1) melatonin has anti-inflammatory, antioxidant, immunomodulatory, and Mpro and MMP9 protein-inhibitory activity. (2) It has been shown to have a wide margin of safety. (3) The contributions reviewed make it an effective therapeutic alternative in the treatment of SARS-CoV-2 infection. (4) Further clinical trials are recommended to clearly define the administration protocol.
The SARS-CoV-2 virus can within days move from the respiratory system into the brain, heart, and nearly every organ system in the body, and stay there for months, a new study says. A team from the US National Institutes of Health (NIH) described their research as the “most comprehensive analysis” to date of how the virus spreads through the human body. The results were published online on Saturday in a manuscript, which was submitted under review in the Nature journal. The scientists based their findings on autopsies of 44 patients who died after contracting Covid. The autopsies were performed between April 26, 2020 and March 2, 2021. “Our results collectively show while that the highest burden of SARS-CoV-2 is in the airways and lung, the virus can disseminate early during infection and infect cells throughout the entire body, including widely throughout the brain.”
The viral RNA was “widely distributed” even among patients who died with asymptomatic or mild cases of Covid, the researcher wrote. In some instances, the virus stayed in “regions throughout the brain” for up to 230 days following symptom onset. Ziyad Al-Aly, the director of the clinical epidemiology center at the Veterans Affairs St. Louis Health Care System in Missouri, told Bloomberg the study may provide an answer to why some patients suffer from so-called ‘long Covid’, when symptoms stay persistent for months. “For a long time now, we have been scratching our heads and asking why long Covid seems to affect so many organ systems. This paper sheds some light, and may help explain why long Covid can occur even in people who had mild or asymptomatic acute disease,” Al-Aly said.
Dr. Pierre Kory is one of the leaders in the movement to provide early treatment for COVID infection. Kory is a critical care physician (ICU specialist), triple board certified in internal medicine, critical care and pulmonary medicine, and is part of the Frontline COVID-19 Critical Care Alliance (FLCCC), which was among the first to publish COVID treatment guidance. Kory spent most of his career at the Beth Israel Medical Center in Manhattan, New York, where he helped run the intensive care unit. He also had a busy outpatient practice. About six years ago, he was recruited to the University of Wisconsin Medical Center in Milwaukee, Wisconsin, where he led the critical care service. “When COVID hit, I was in a leadership position,” he says. “I resigned, because of the way they were handling the pandemic.”
University of Wisconsin Medical Center, like most hospitals across the U.S., insisted on providing supportive care only, and Kory refused to remain in a leadership position under those circumstances. Patients were, for the first time in modern medical history, told to just suffer at home until they were near death, then go to the hospital where they were placed on deadly ventilator treatment. “I knew there was a variety of treatments that we could use [yet] we were using nothing,” he says. Doctors were even told to not use anticoagulants, even though blood clotting was “through the roof” in many patients. “You could draw blood and actually see the blood clotting very quickly in the tubes,” he says. Since those early days, the disease seems to have changed considerably. We don’t see the high rates of blood clotting anymore, for example, which is good news.
But for some reason, from the very start, “they were literally telling us that we needed randomized controlled trials to do anything,” Kory says, and to this day, health authorities are refusing to acknowledge any treatment protocol outside of the drug remdesivir, and COVID vaccins. “People were dying, [yet] all of my ideas were getting shouted down. My superiors were showing up [to my clinical meetings] and getting me to stand down, because I was entertaining the idea that we should do this, that and the other thing, and they didn’t want anything to be done. And so, I said, ‘I’m done.’ I resigned mid-April 2020. I then went to New York for five weeks and ran my old ICU in New York.”
In May 2020, Kory testified before the U.S. Senate, stressing how critical it was to use steroids during the hospital phase of this infection. At that time, he was still employed by the University of Wisconsin. His resignation date had not yet happened, and they “were livid that I was speaking in public, giving my opinion.” This is remarkable, because when you’re an expert in a field, “you’re actually responsible to share your insight and expertise,” Kory says. “Yet they were very unhappy that I was doing that.” Seven weeks later, Kory was vindicated when the British Recovery trial results came out, showing the benefits of corticosteroids. Since then, steroids have become part of standard of care in the hospital phase.
Steroids are an effective tool for reducing inflammation in general, but they appear particularly important for advanced COVID infection. I had a close friend who contracted a very serious case of COVID-19 and kept worsening despite taking everything I suggested. He knew Dr. Peter McCullough, so he texted him and was told to add prednisone and aspirin to his current regimen. As soon as he took the prednisone, he started getting better. As explained by Kory, this is a common experience. Importantly, the evidence shows that when used early, during mild infection, corticosteroids do more harm than good. But once you are entering into moderate illness, as soon as you start to see lung dysfunction or the need for oxygen, steroids are critical and are clearly lifesaving.
Reality is penetrating the fog and fury of propaganda spewed out over cable-TV news in what may be the last desperate full-out campaign to sell “vaccines” to the credulous. Omicron is a bust, despite the shrieking about overstuffed hospitals (they’re not) in The New York Times. Just as there is a crack-up boom in the final stage of a financial crisis, there is a climactic surge of hysteria in the Covid-19 war against Western Civ. Now, Dr. Anthony Fauci is pushing proof-of-vaxx for US air travel because, “[a] vaccine requirement for a person getting on the plane is just another level of getting people to have a mechanism that would spur them to get vaccinated…” he laid it out on ABC News’s This Week show Sunday with Jonathan Karl.
Monday morning on NPR, Dr. Fauci was beating the drum about the unvaxxed being a menace to society as maxi-spreaders of omicron. Is it possible he hasn’t heard that the vaxxed are catching it at a greater rate despite their vaxxes than the unvaxxed? Do you know why? Because their previous vaxxes have de-tuned their immune systems, that’s why. By the way, so far, one death has been attributed to omicron in the US — and even that case is a muddle. And Dr. Fauci is beseeching the twice-vaxxed to go get boostered? Is he determined to wreck absolutely every immune system in the land? Kind of looks that way, a little bit.
I confess I am torn between two views of this fiasco. The first is that the notoriously incompetent Dr. Fauci and his colleagues (read RFK, Jr.s book) simply blundered through the Covid-19 disaster making a series of reckless choices, and about halfway through the crisis made the dastardly decision to cover-up their errors by doubling and tripling down on these mistakes. For instance, the policy to suppress and ban cheap and effective treatments that would have un-horsed their stupendously profitable “vaccines” from the emergency use authorization that got the mRNA cocktails into the public’s arms without proper testing. Some months down the road we will learn that this Fauci combine caused millions of people to die unnecessarily both from treatments withheld and from the adverse effects of vaxxes themselves.
The other view — that is becoming ever-harder to disregard — is that the Covid-19 pandemic was a deliberate program by a gang of powerful international adventurers to install a regime of surveillance and extreme control over formerly free citizens — all in the service of “re-setting” the ailing global financial system, reducing the population of elder pensioners to relieve the West’s payment obligations, and stifling industrial economies as a cure for climate change. It has sounded a little preposterous to me that such manifest evil, as otherwise seen only in James Bond movies and newsreels of the Nazis, could actually be true.
Despite there being no chemical or ethical differences between Comirnaty and Pfizer-BioNTech, however, the FDA acknowledges the two “are legally distinct.” The agency explained in a statement to the Ohio Star that statutory authorities governing EUAs and biologics license applications, which are necessary for official FDA approval, “provide different legal requirements.” Those requirements, such as more paperwork for a full approval, mean the two products are labeled differently. Labeling differences, while important for the company, mean little in practice for those receiving the vaccine, explained Riley. But legal differences between the EUA-sanctioned and FDA-approved vaccines have potentially significant implications for vaccine mandates.
The Department of Defense, for example, mandates that service members become fully vaccinated against COVID-19 but directs that only FDA-approved vaccines be used for mandatory vaccination. (Service members may also volunteer to receive a EUA vaccination to meet the requirement.) And in Ohio, a recently signed law states that “a public school or state institution of higher education shall not … require an individual to receive a vaccine for which the [FDA] has not granted full approval.” Such measures have led to debates over the precise nature of the legal differences between the two types of vaccines — and whether FDA approval should legally be a limitation for vaccine mandates. R. Davis Younts, an attorney based in Lemoyne, Penn., who represents dozens of clients resisting vaccine mandates, said the government can’t compel people to take vaccines that have only been authorized under EUA.
“Government agencies do not have the legal authority to mandate any of the EUA vaccines,” Younts told Just the News. He explained how Section 564 of the Federal Food, Drug, and Cosmetic Act requires that vaccine recipients must be informed of “the option to accept or refuse” the product. Younts, focusing on military personnel, added that, in order to make an EUA drug mandatory, the president must issue a waiver under a certain federal statute. That statute states, “Administration of a product authorized for emergency use under section 564 … to members of the armed forces” requires informed consent absent a determination by the president that “complying with such requirement is not in the interests of national security.”
U.S. health officials on Monday cut isolation restrictions for asymptomatic Americans who catch the coronavirus from 10 to five days, and similarly shortened the time that close contacts need to quarantine. Centers for Disease Control and Prevention officials said the guidance is in keeping with growing evidence that people with the coronavirus are most infectious in the two days before and three days after symptoms develop. The decision also was driven by a recent surge in COVID-19 cases, propelled by the omicron variant. Early research suggests omicron may cause milder illnesses than earlier versions of the coronavirus. But the sheer number of people becoming infected — and therefore having to isolate or quarantine — threatens to crush the ability of hospitals, airlines and other businesses to stay open, experts say.
CDC Director Rochelle Walensky said the country is about to see a lot of omicron cases. “Not all of those cases are going to be severe. In fact many are going to be asymptomatic,” she told The Associated Press on Monday. “We want to make sure there is a mechanism by which we can safely continue to keep society functioning while following the science.” Last week, the agency loosened rules that previously called on health care workers to stay out of work for 10 days if they test positive. The new recommendations said workers could go back to work after seven days if they test negative and don’t have symptoms. And the agency said isolation time could be cut to five days, or even fewer, if there are severe staffing shortages.
Now, the CDC is changing the isolation and quarantine guidance for the general public to be even less stringent. The change is aimed at people who are not experiencing symptoms. People with symptoms during isolation, or who develop symptoms during quarantine, are encouraged to stay home. The CDC’s isolation and quarantine guidance has confused the public, and the new recommendations are “happening at a time when more people are testing positive for the first time and looking for guidance,” said Lindsay Wiley, an American University public health law expert. Nevertheless, the guidance continues to be complex.
Between heaven and Earth, where do aliens fit in? That’s the question that NASA hopes theologians at the Center for Theological Inquiry (CTI) in Princeton, New Jersey, can answer, in a recent effort to understand how humans will react to news that intelligent life exists on other planets. University of Cambridge religious scholar Rev. Dr. Andrew Davison, who also holds a doctorate in biochemistry from Oxford, is one of the 24 theologians enlisted to help with the project, the Times UK reported last week. In a recent statement on the University of Cambridge’s Faculty of Divinity blog, Davison says his research so far has already seen “just how frequently theology-and-astrobiology has been topic in popular writing” during the previous 150 years.
Davison’s upcoming book, “Astrobiology and Christian Doctrine,” due out in 2022, according to the Times, will cover part of CTI and NASA’s joint spiritual exploration, in which his “most significant question” is how theologians would respond to the notion “of there having been many incarnations [of Christ]” in the universe, he added in the blog post. This is the latest dispatch to come in a partnership between the US space agency and the religious institute. In 2014, NASA awarded CTI a $1.1 million grant to study worshippers’ interest in and openness to scientific inquiry called the Societal Implications of Astrobiology study. Studies have shown links between religiosity and belief in extraterrestrial intelligence.
Research published in 2017 found that people with a strong desire to find meaning, but a low adherence to a particular religion, are more likely to believe aliens exist — indicating that faith in either theory may come from the same human impulse. With NASA’s support, CTI’s director Will Storrar said they’d hoped to see “serious scholarship being published in books and journals” to come out on the subject, answering to the “profound wonder and mystery and implication of finding microbial life on another planet.” According to the Times, Davison’s book notes that a “large number of people would turn to their religions traditions for guidance” if extraterrestrials were found, and what that means “for the standing and dignity of human life.”
A virus so strong that it can get past 3 vaccines but can’t get past your paw patrol mask.
Being in a minority, even in a minority of one, did not make you mad. There was truth and there was untruth, and if you clung to the truth even against the whole world, you were not mad.
– George Orwell, 1984
Billy Connolly – Politically correct – Was it something I said?
Elon Musk- Bill
Support the Automatic Earth in virustime with Paypal, Bitcoin and Patreon.
Jules Adler Panorama de Paris vu du Sacré Coeur 1935
Sometimes the best information comes from unexpected sources. That is certainly true this weekend. Spectator Editor Fraser Nelson had a very revealing Twitter talk with Graham Medley, chair of COVID modeling for UK Government’s Scientific Advisory Group for Emergencies (SAGE). But first, to get in the mood, a graph on Omicron from South Africa, because that’s what they’re all talking about:
And if you don’t find that convincing (because it’s “only” South Africa), Robert Malone has your back with his take on a Danish study.
Denmark, as of December 9, 2021. Denmark has one of the highest RT-PCR testing capacities in the world and screens all positive RT-PCR tests with an Omicron-specific PCR – allowing screening for Omicron. There have been 785 SARS-CoV-2 Omicron variant cases identified in Denmark. The earliest Omicron cases in Denmark occurred before South Africa announced the emergence of this variant. Most cases were fully (76%) or booster-vaccinated (7.1%); 34 (4.3%) had a previous SARS-CoV-2 infection. The majority of cases with available information reported symptoms (509/666; 76%) and most were infected in Denmark (588/644; 91%). One in five cases cannot be linked to previous cases, indicating widespread community transmission. Nine cases have been hospitalized, one required intensive care and no deaths have been registered.
Highlights: · 1.2% of cases have been hospitalized
· 0.3% in intensive care
· 0% deaths.
· 83% were fully or booster vaccinated, 17% not vaccinated (including 2.6 vaccine started)
· 4.3% had previous SARS-CoV-2 infection
· 91% have no travel history, 9% reported travel
My take: this study is important because although there are studies and spokespeople from South Africa stating similar results, the Danish population in terms of age, body weight, life expectancy, etc. is more similar demographically to the US population. This Danish study suggests that Omicron will affect the American population similarly.
I wrote earlier today: “Mild” is a four letter word. Well, for politicians and media and drugmakers, that is.
Then, the UK. Where word today is that 12 people have died WITH Omicron and 104 are in hospital WITH Omicron. Dying WITH Omicron is not the same as dying FROM Omicron, and being in hospital with it says nothing either, if you don’t know a patient’s age, history, comorbidities etc. And a “case”, as that word is abusively used all the time, is in reality just a positive test with the inherently flawed PCR procedure, and 99.7% of positive tests never go anywhere. Meaningless.
The UK Government’s Scientific Advisory Group for Emergencies, SAGE, predicts “anything from 200 to 6,000 deaths a day” (42,000 a week) from Omicron, and I read somewhere there’s a 2 million cases per week prediction. But there’s something about SAGE’s working methods that you really should know: they only focus on bad or worse scenarios. And it’s not even strictly their fault: good or mild scenarios are simply not their assignment.
Here are Spectator Editor Fraser Nelson and SAGE chair of COVID modeling Graham Medley:
The latest Sage papers have been published, envisaging anything from 200 to 6,000 deaths a day from Omicron depending on how many more restrictions we’ll get – up to and very much including another lockdown. Earlier today I had an unexpected chance to ask questions of Graham Medley, the chair of the Sage modelling committee. He’s a professor at London School of Hygiene & Tropical Medicine (LSHTM) which last weekend published a study on Omicron with very gloomy scenarios and making the case for more restrictions. But JP Morgan had a close look at this study and spotted something big: all the way through, LSHTM assumes that the Omicron variant is just as deadly as Delta. ‘But evidence from South Africa suggests that Omicron infections are milder,’ JP Morgan pointed out in a note to clients. Adjust for this, it found, and the picture changes dramatically:-
“Bed occupancy by Covid-19 patients at the end of January would be 33% of the peak seen in January 2021. This would be manageable without further restrictions.’ So JP Morgan had shown that, if you tweak one assumption (on severity) then – suddenly – no need for lockdown. Why was this scenario left out? Why would this fairly-important and fairly-basic fact on Omicron modelling not presented by SAGE modellers like Prof Medley to ministers – and to the general public? I was thrilled for the chance to speak to him on Twitter. It was kind of him to make the time (he’s still going, as far as I can make out). The Spectator data hub has a page devoted to past Sage modelling vs actual, and I wanted to make sure I was not being unfair to Sage in my selection or presentation of those charts.
The latest Sage paper-drop – the 6,000-deaths-a-day one – refers to ‘scenarios,’ not predictions. Prof Medley emphasises the distinction: saying something could happen is not saying that there’s a realistic chance of it happening. But then why do SAGE modellers publish some scenarios and not others? I then jumped to ask Prof Medley.
Revealingly, he seemed to think my question odd: if it’s quite plausible that Omicron is mild and doesn’t the threaten the NHS, what would be the point of including that as a ‘scenario’? He seemed to suggest that he has been given a very limited brief, and asked to churn out worse-case scenarios without being asked to comment on how plausible they are. “We generally model what we are asked to model. There is a dialogue in which policy teams discuss with the modellers what they need to inform their policy.” Might this remit mean leaving out just-as-plausible, quite-important scenarios that would not require lockdown? “Decision-makers are generally on only interested in situations where decisions have to be made.”
Note how careful he is to stay vague on whether any of the various scenarios in the Sage document are likely or even plausible. What happened to the original system of presenting a ‘reasonable worse-case scenario’ together with a central scenario? And what’s the point of modelling if it doesn’t say how likely any these scenarios are? From what Prof Medley says, it’s unclear that the most-likely scenario is even being presented to ministers this time around. So how are they supposed to make good decisions? I highly doubt that Sajid Javid is only asking to churn out models that make the case for lockdown. That instruction, if it is being issued, will have come from somewhere else.
Isn’t that the craziest thing? I think Nelson may be right, and politicians may not be looking for deliberately misleading (to the downside) studies. But those are still all they get, and base their policies upon.
And for some people involved, I am not so sure. Like for Anthony Fauci, and for Pfizer. And of course, the problem with SAGE modeling is probably repeated in 100 other countries, by all the so-called experts, and they feed off each other. Count your blessings.
Meanwhile, the UK increased its PCR testing by some 65% recently, so what are we really talking about, if not apples and bananas?
Reported infections in the U.K. have suddenly spiked in the last three days, up from 59,610 on Tuesday to 78,610 on Wednesday, 88,376 on Thursday and 93,045 on Friday. Looking at the data regionally, the spike is currently much more pronounced in London, the South East, the East of England, the East Midlands and the North West than it is in the North East, Yorkshire and the Humber, the South West and the West Midlands. It’s not clear at this point if it is going to continue to rise, though the last three days’ counts don’t appear to indicate continued sharp growth. It is also so far largely an artefact of massively increased testing, as the graph below with data for the U.K. up to December 16th shows. Similar is true for Scotland. Positive tests have spiked.
But positivity is up only a little due to the large increase in testing. How significant is it that the spike began on Monday December 13th, the day after Boris Johnson’s Sunday press conference when he warned everyone about Omicron and told them to get their booster jab? There was a huge surge in demand for booster doses starting that Monday and continuing throughout the week. Could the fact that this surge coincided with a similar surge in both testing and positive tests be more than coincidence? Perhaps people got tested before getting their booster, or just because of the dire warning of a new threat.
The CDC doesn’t like the term “mild”, and neither do the media. because it makes for poor clickbait. They all prefer terms like “grim”, “soar”, “rocket”, “leap”. And they love the words “patients” and “deaths”. As US deaths were down by, what, 30%? (Note in the graph how deaths decreased).
Grim new figures from the Centers for Disease Control and Prevention (CDC) have predicted that US COVID-19 deaths will soar by 73 per cent to 15,600 a week by January 8, and that cases will rocket to 1.3 million a week by Christmas Day. The agency revealed projections on Wednesday afternoon that show America will suffer up to 15,600 new Covid deaths a week as of January 8 – or 2,228 deaths per day – a 58 per cent increase from 8,900 deaths currently being recorded each week, equivalent to 1,285 deaths a day. Another CDC prediction estimates that between 620,000 and 1.3 million Americans will have been diagnosed with Covid by the week that ends on December 25 – Christmas Day. That represents a 55% leap on the 840,000 cases that have been recorded over the last week.
Omicron will likely become the dominant Covid strain in the coming weeks, and cause a massive surge of cases shortly after Christmas, one expert has warned, likely fueling the surge the CDC predicts. Dr Gregory Poland, a top epidemiologist at the Mayo Clinic told DailyMail.com that an Omicron-fueled surge in cases could be right around the corner. ‘As best any of us can model, we will have an explosion of cases after the holidays in the in the early-to-mid-January timeframe,’ he said. ‘This variant is hyper transmissible, it spreads exponentially in an environment of cold weather, massive holiday get togethers, no masking and insufficient immunization.’
He believes it will become the dominant strain in the UK – which recorded a record 78,610 cases on Wednesday – in the coming days, and that the U.S. will follow around two weeks later. Cornell University in upstate New York is suspected to be home to the first US Omicron cluster, after 930 students were diagnosed with the virus in recent days. The college says every one of the positive tests it has sequenced so far has been the Omicron variant. A Cornell spokesman hasn’t said exactly how many Omicron cases have been identified, but added that they expect most, if not all, the 930 cases to be caused by the new variant.
Anthony Fauci, chief medical advisor to President Joe Biden, said on Sunday that record-breaking death rates could occur as the COVID Omicron variant spreads across the U.S. Fauci made an appearance on CNN’s State of the Union on Sunday, where host Jake Tapper pressed the leading infectious disease expert on where he believes the pandemic is headed. Tapper asked, “Do you expect new record high numbers for cases? And what about hospitalizations and deaths?” “Yes, well, unfortunately, Jake, I think that that is going to happen,” Fauci replied.
“We are going to see a significant stress in some regions of the country on the hospital system, particularly in those areas where you have a low level of vaccination, which is one of the reasons why we continue to stress the importance of getting those unvaccinated people vaccinated.” [..] “It is going to be tough,” Fauci said. “We can’t walk away from that, Jake. We can’t, because, with Omicron that we’re dealing with, it is going to be a tough few weeks to months as we get deeper into the winter.”
If and when you’re suffering under yet another lockdown and/or any other restrictions, you should know they are for naught. There is no indication to date that Omicron will fill up hospitals, or ICUs, or that it will kill millions of people.
But that for now refuted scenario is still why those restrictions are being put in place, why you are being told not to hug your intensely lonely grandma for Christmas. Useless. And why everyone is told to get a booster, and soon another. Also useless.
It’s time for all of you to grow a spine and a pair of balls (sorry, ladies, just a manner of speech) and start living your lives again. Time to get rid of Fauci, and of Pfizer, and SAGE, and fill in your local/national bunch of experts. Because as long as they are there, they will hog the limelight, and you will never be able to start to live your life again.
A simple Christmas message.
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Support the Automatic Earth in virustime. Donate with Paypal, Bitcoin and Patreon.
Interesting short segment from Sky News interviewing the smiling U.K. Health Minister Gillian Keegan about the intense U.K. response to the Omicron variant and the new restrictions announced by government officials. Great Britain is preparing for hundreds-of-thousands of Omicron cases. Video prompted to 05:42 just watch for around 45 seconds. No commentary from me needed. WATCH:
Nations across Europe moved to reimpose tougher measures to stem a new wave of Covid infections spurred by the highly transmissible Omicron variant, with the Netherlands leading the way by imposing a nationwide lockdown. All non-essential stores, bars and restaurants in the Netherlands will be closed until 14 January starting Sunday, caretaker prime minister Mark Rutte said at a hastily arranged press conference Saturday night. Schools and universities will shut until 9 January, he said. In what is surely to prove a major disappointment, the lockdown terms also rein in private holiday celebrations. Residents only will be permitted two visitors except for Christmas and New Year’s, when four will be allowed, according to Rutte.
“The Netherlands is going into lockdown again from tomorrow,” he said, adding that the move was “unavoidable because of the fifth wave caused by the Omicron variant that is bearing down on us.” It wasn’t just the Dutch seeking to slow the spread of Omicron. Alarmed ministers in France, Cyprus and Austria tightened travel restrictions. Paris canceled its New Year’s Eve fireworks. Denmark has closed theatres, concert halls, amusement parks and museums. Ireland imposed an 8 pm curfew on pubs and bars and limited attendance at indoor and outdoor events. London mayor Sadiq Khan underscored the official concern about the climbing cases and their potential to overwhelm the health care system by declaring a major incident Saturday, a move that allows local councils in Britain’s capital to coordinate work more closely with emergency services.
Irish prime minister Micheal Martin captured the sense of the continent in an address to the nation, saying the new restrictions were needed to protect lives and livelihoods from the resurgent virus. “None of this is easy,” Martin said Friday night. “We are all exhausted with Covid and the restrictions it requires. The twists and turns, the disappointments and the frustrations take a heavy toll on everyone. But it is the reality that we are dealing with.”
Reported infections in the U.K. have suddenly spiked in the last three days, up from 59,610 on Tuesday to 78,610 on Wednesday, 88,376 on Thursday and 93,045 on Friday. Looking at the data regionally, the spike is currently much more pronounced in London, the South East, the East of England, the East Midlands and the North West than it is in the North East, Yorkshire and the Humber, the South West and the West Midlands. It’s not clear at this point if it is going to continue to rise, though the last three days’ counts don’t appear to indicate continued sharp growth. It is also so far largely an artefact of massively increased testing, as the graph below with data for the U.K. up to December 16th shows. Similar is true for Scotland. Positive tests have spiked.
But positivity is up only a little due to the large increase in testing. How significant is it that the spike began on Monday December 13th, the day after Boris Johnson’s Sunday press conference when he warned everyone about Omicron and told them to get their booster jab? There was a huge surge in demand for booster doses starting that Monday and continuing throughout the week. Could the fact that this surge coincided with a similar surge in both testing and positive tests be more than coincidence? Perhaps people got tested before getting their booster, or just because of the dire warning of a new threat.
We would normally expect a spike in winter viral illness at this point in December, so there is nothing particularly unusual about it. In this regard, it’s worth noting that the Covid deaths trend for the U.K. is currently very similar to normal winter flu deaths at this time of year. However, the recent announcement of the Omicron variant raises the question of the role it might be playing in the surge.
Background: Ivermectin has demonstrated different mechanisms of actions that could potentially protect from both COVID-19 infection and COVID-19-related comorbidities. Based on the existing literature and safety profile of ivermectin, a citywide program of prophylactic use of ivermectin for COVID-19 was implemented in Itajai, a Southern city in Brazil in the state of Santa Catarina. The objective of this analysis is to evaluate the effects of the use of ivermectin for prevention of COVID-19 infection, risk of dying and mortality, compared to non-users.
Materials and methods: This is a retrospective analysis of registry data from the medical based citywide COVID-19 prevention with ivermectin program, between July 2020 to December of 2020. The whole population of Itajaí was invited for a medical visit to compile demographic and medical parameters. In the absence of contraindications, ivermectin was offered as an optional treatment for 2 days every 15 days at a dose of 0.2mg/kg/day. Patients’ preferences and medical autonomy were preserved. Ivermectin users were compared with the comorbidity-matched population of non-users for COVID-19 by age, sex, COVID-19 infection rate, and COVID-19 mortality rate. Results in terms of mortality were adjusted for all relevant variables and Propensity Score Matching (PSM) was calculated.
Results: A total of 220,517 subjects were included in the analysis; 133,051 (60.3%) ivermectin users and 87,466 (39.7%) non-users. COVID-19 infection occurred in 4,311 (3.2%) treated subjects, and 3,034 (3.5%) non-treated subjects. This evidence showed a 7% reduction in COVID-19 infection rate with use of ivermectin: COVID-19 infection rate ratio (Risk ratio (RR) of 0.93; 95% confidence interval (CI), 0.89 – 0.98; p = 0.003). A total of 62 deaths (1.4% mortality rate) occurred among users and 79 deaths (2.6% mortality rate) among non-users, showing a 48% reduction in mortality rate (RR, 0,52; 95%CI, 0.37 – 0.72; p = 0.0001). Risk of dying from COVID-19 among ivermectin users was 45% lower than non-users (RR, 0.55; 95%CI, 0.40 – 0.77; p = 0.0004).
Conclusion: Prophylactic use of ivermectin showed significantly reduced COVID-19 infection rate, mortality rate and chance of dying from COVID-19 on a calculated population-level analysis, which controlled for all relevant confounding variables.
Prophylactic ivermectin works (new study just published): "Risk of dying from COVID-19 among ivermectin users was 45% lower than non-users" https://t.co/BMIFSRIKhB
“..or we can take every little mutation and every little change and try to make it into a crisis so we can frighten people and control their lives more..”
“We’ve been having tunnel vision” dealing with the COVID-19 pandemic, Dr. Ben Carson told EpochTV’s “American Thought Leaders” program. “Let’s throw the politics out. We could solve this problem pretty quickly,” he stated in an interview that will premiere on Dec. 18 at 7 p.m. New York time. “Let’s open this thing up to all the different mechanisms,” said Carson, a renowned neurosurgeon who was awarded the Presidential Medal of Freedom—the highest civilian award in the nation—in 2008 for his work. He retired in 2013 and ran for the presidency in 2016, before serving as the secretary of Housing and Urban Development during the Trump administration.
“Let’s look around the world at things that work. Let’s look at the fact that on the western coast of Africa, there’s almost no COVID. And let’s ask ourselves, why is that? And then you see, it’s because they take antimalarials, particularly hydroxychloroquine. Let’s study that. Let’s see what’s going on there. “Let’s listen to these physician groups who’ve had incredible success with ivermectin. Let’s look at the results with monoclonal antibodies. Let’s look at all of these things. Let’s put them all in our armamentarium so that we don’t have a one-size-fits-all system.” The U.S. Food and Drug Administration (FDA) at one time had authorized hydroxychloroquine for treating certain COVID-19 patients but quickly revoked the emergency use authorization (EUA) in June 2020, claiming no data showed its effectiveness.
The FDA hasn’t approved or issued an EUA for ivermectin to treat COVID-19, citing the same reasons. Using hydroxychloroquine or ivermectin to treat COVID-19 patients has been highly controversial. Some studies show, and some doctors claim, that hydroxychloroquine or ivermectin can effectively treat COVID-19 patients. A vaccine confidence insight report (pdf) from the Centers for Disease Control and Prevention (CDC) labeled such claims as misinformation or disinformation. “COVID is a virus. Viruses mutate. That’s what they do. And they will continue to mutate,” Carson said. Carson pointed out that fortunately, most of the time, viruses become a little weaker with each mutation. “We can admit that and deal with it, or we can take every little mutation and every little change and try to make it into a crisis so we can frighten people and control their lives more,” Carson said.
The federal agencies in charge of COVID-19 response are taking hits from former officials and high-profile medical professors for “sidelining experts,” not conducting basic research, and mischaracterizing evidence related to vaccines and masks for young people. The Biden administration is getting a pass for “extreme political pressure” that “appropriately” prompted outrage against its predecessor, two FDA alumni wrote in The Washington Post Thursday. Former Office of Vaccines Research and Review Deputy Director Philip Krause and former acting Chief Scientist Luciana Borio protested three recent actions authorizing boosters for people as young as 16.
“Before last month, the standard practice was for the agencies to convene standing outside advisory committees, whose members inspect the relevant data, debate it and vote,” they wrote. Earlier debates and votes suggest that “at least some experts would probably have voiced opposition,” and the refusal to hear them out “could hurt the credibility of these agencies.” They criticized the FDA’s “unpersuasive” explanation that authorizing boosters for 16- and 17-year-olds “does not raise questions that would benefit from additional discussion by committee members.” Exigency is “the exact circumstance when expert discussion and interpretation of the data can make the biggest difference,” the duo wrote.
Krause left the FDA in apparent protest of the White House sidestepping the agency to promise booster shots across the board. He soon joined a public letter warning “there could be risks if boosters are widely introduced too soon, or too frequently,” with implications for “vaccine acceptance.” The White House is “acting seriously reckless,” University of California San Francisco medical professor Vinay Prasad tweeted, echoing Krause’s argument. “If the last administration did this, all experts would be outraged. Principles only matter when they are inconvenient.”
Johns Hopkins University medical professor Marty Makary, who agrees boosters can harm low-risk groups, blasted the feds for too much “speculation” and too little research on the Omicron variant, just their latest pandemic failure. “In fact, most of our COVID findings have come from Israel and scientists abroad,” he wrote in a New York Post op-ed Dec. 8 decrying “turtle-speed bureaucracy.” It’s baffling that the National Institutes of Health or CDC has not “mobilize[d] any of their 7,000-plus scientists” to quickly answer how antibodies from vaccines and natural immunity respond to Omicron, said Makary, editor-in-chief of MedPage Today. There’s not even a “real-time data dashboard” on Omicron cases.
“Perhaps [Anthony] Fauci could have done fewer media interviews and university lectures … and instead personally overseen an NIH Omicron-antibody-binding experiment,” he said. Makary blasted the CDC for consistently releasing “tardy and incomplete data, missing key information on risk stratification, the role of obesity and a breakdown of child deaths by comorbidity as we imposed blanket restrictions on 72 million children.”
Pfizer Inc said on Friday the Covid-19 pandemic could extend through next year and announced plans to develop a three-dose vaccine regimen for children ages 2 to 16, a move that could delay its authorisation. The US pharmaceutical company made its comments as European countries geared up for further travel and social restrictions and a study warned that the rapidly spreading Omicron coronavirus variant was five times more likely to reinfect people than its predecessor, Delta. Pfizer executives said the company believed that by 2024, the disease should be endemic around the globe, meaning it would no longer be a pandemic. The company projected that “Covid will transition to an endemic state potentially by 2024.”
Prior to the Omicron variant, top US disease doctor Anthony Fauci forecast the pandemic would end in 2022 in the United States. Announcing plans to develop a three-dose regimen for ages 2 to 16, Chief Scientific Officer Mikael Dolsten told a conference call that results of three doses among people older than 16 showed that approach offered greater protection. “Therefore, we have decided to modify each of the pediatric studies to incorporate a third dose to the series and seek licensure for a three-dose series rather than a two-dose series as originally anticipated,” the company said.
Pfizer developed its Covid-19 vaccine with Germany’s BioNTech SE. The companies have been developing a version of their vaccine tailored to combat the Omicron variant, but have not decided whether it will be needed. They expect to start a clinical trial for the updated vaccine in January, the Pfizer executives said. The risk of reinfection with the Omicron variant is 5.4 times higher and it shows no sign of being milder than the Delta variant, a study by Imperial College London found, as cases soar across Europe and threaten year-end festivities. Past infection may offer as little as 19% protection against reinfection by the new variant, Imperial College said, noting that the study of hundreds of thousands of cases, including 1,846 confirmed as Omicron, had not been peer reviewed.
Dr. Anthony Fauci and the head of the National Institute of Health (NIH) colluded on a way to discredit an alternative plan to deal with COVID from a group of experts, released emails reveal. The emails, some of which were tweeted out on Saturday by Phil Magness, senior research faculty and interim research and education director at the American Institute for Economic Research (AIER), show Fauci and Francis Collins attempting to coordinate a ‘devastating takedown’ of the Great Barrington Declaration. AIER, a libertarian think tank, sponsored the declaration, which largely abandons lockdowns in favor of a herd immunity strategy that allows life to return to normal.
In an October 8 email from Collins to Fauci, the head of the NIH calls the GBD the work of ‘three fringe epidemiologists’ that ‘seems to be getting a lot of attention.’ Collins adds that ‘there needs to be a quick and devastating published takedown of its premises. I don’t see anything like that online yet – is it underway?’ Later in the day, Fauci sends Collins a Wired op-ed that refutes the notion of herd immunity stopping the pandemic. Collins then sends Fauci an op-ed in The Nation also trashing the GBD.
A few days later, Collins emails Fauci a Washington Post op-ed he’s quoted in headlined ‘Proposal to hasten herd immunity to the coronavirus grabs White House attention but appalls top scientists.’ Collins – working under former President Donald Trump at the time – said ‘my quotes are accurate but will not be appreciated in the [White House].’ Fauci responds: ‘They are too busy with other things to worry about this. What you said was entirely correct.’ Later, Gregg Gonsalves – the writer of The Nation op-ed – sends Collins an email thanking him with a subject line that includes saying legendary AIDS activist Larry Kramer ‘would be proud.’ Collins responds with a smiley face.
The GBD – authored by previous DailyMail.com contributor Jay Bhattacharya of Stanford University, Sunetra Gupta of the University of Oxford and Martin Kulldorff of Harvard University, calls for individuals at significantly lower risk of dying from COVID-19 – as well as those at higher risk who so wish – to be allowed ‘to resume their normal lives.’ That would mean allowing people in low risk groups to go to offices, hang out in bars and restaurants and go to sporting and entertainment events. The centerpiece of the declaration, according to Dr. Bhattacharya, is a call for increased focused protection of the vulnerable older population, who are more than a thousand times more likely to die from COVID infection than the young. The declaration makes no mention of social distancing, masks, tracing, or long-term Covid cases but suggests that increased infection of those at lower risks would build herd immunity.
Had it not been for the likes of McCullough, Fareed, Zelenko, Tenenbaum, Oskoui, Urso, Littell, Malone, Vanden Bossche, Yeadon, Ryan Cole, Kulvinder Gill, Francis Christian, Trozzi, Phillips, Palmer, Hodkinson, Bhattacharya, Heneghan, Kulldorff, Bridle, Mallard, Bernstein, Risch etc. to me, take the whole lot of the million doctors and fire them all…every one damn of them, they have caused this by being silent and being on the take…yes, I know many from CDC and NIH and even FDA who told me they cant speak out because of fear of losing their appointment and grant…yes, this be about money…grift and graft…they have all benefitted and of course the top dog Bourla of Pfizer with his buddy Fauci…imagine this grifter Bourla saying we are criminals because we question the efficacy and safety of the vaccines…this piece of untermensche s***….
The Canadian and UK and American doctor, yes Kuntsler, have shown themselves to be among the most dweeb, pusillanimous, weak, cowardly, craven, money hungry, grifters, stiff necked idiots and fools…money whores to the pharma…selling out the good populations for benefit to yourself…you sick twisted set of doctors…you dont see it yet but your gravitas id now DOA…and you did it to you. you had it all and now are worth nothing. you helped destroy your careers, your name, EBM, research, all of it…you did this…you joined a devious scheme and history will recall and remind you always of what you did. you are utterly corrupt and I tell you in your face here…corrupt untermensche.
Yes it the doctors we used to revere and admire, that have lost all credibility along with the entire research establishment, the medical publication process, the journal editors, all of them were and are on the take in some manner…their silence got them something and we will come to learn in time…fire these bastards, all of them. These losers oh I meant doctors and scientists in the US and Canada and UK etc…sucking on the teats of NIH grants and CIHR grants…losers the whole bunch of them should hang heads in shame…abject failures….it is their disastrous unscientific illogical and specious policies that have harmed populations…children hung themselves and it was this Trump was fighting against and Atlas…I know I was there. Atlas did many things to stem the tide of the massive deaths in the nursing homes and deserves big credit…I know, I was there.
America has some of the most advanced medical research capabilities in the world. So why is it that a small group of labs in South Africa seems to be a step ahead of everybody else when it comes to sniffing out new variants? The group first gained notoriety for discovering the beta variant and alerting the world to its presence. But most people probably became familiar with Alex Sigal, Tulio de Oliveira and their work at a gene-sequencing laboratory in the South African port city of Durban when they announced the discovery of the omicron variant, the latest “variant of concern” while Americans were enjoying their Thanksgiving dinner. What is it that makes their lab so successful? Well, it looks like Bloomberg has finally found the answer in a profile of the Africa Health Research Institute, as it’s formally known.
South African scientists became experts at combating viruses almost by necessity, They have been hard at work fighting AIDS, Turburculosis and other viruses – work that has made them a magnet for the world’s best epidemiologists. Because of this, Sigal’s lab has become a kind of training ground for scientists across the continent. It was the first to test omicron against blood plasma from people who’d received two doses of the Pfizer jab. They also developed a theory claiming that immunodepressed people might be breeding grounds for mutants since they’re so vulnerable. One reason for its success with finding new variants: South Africa has set up a network of seven genomic surveillance labs with one at the National Institute for Communicable Diseases and six at academic institutions. Sigal works with Tulio de Oliveira, the Brazilian head of the gene-sequencing laboratory Krisp.
“There’s a lot of technical capacity in South Africa to do genomic sequencing of pathogens because we’ve built up that expertise over many years for HIV and TB,” said Richard Lessells, a Scottish infectious diseases specialist at Krisp. “Very early on in the pandemic, we recognized that genomic sequencing and genomic surveillance was going to be very important.” Since the discovery of omicron, many of the scientists working in the lab have been dealing with sleepless nights. “I’ve been working to get the Pfizer vaccine efficacy study ready,” said Sigal, who becomes animated when he watches a time-lapse video of the omicron variant attacking cells. “I worked through the night.” Put another way: the more variants they “discover”, the more prestige and funding they will be rewarded with.
“..CDC data show 240MM people with at least one shot – about 72.5% of the population. But it also says only 203MM have been fully vaccinated, or 61.3%..”
What a surprise – the CDC and states across the country have been over-counting the number of American adults who have been fully vaccinated. Here’s how Bloomberg explains this accident (because what kind of person would do this on purpose?): “in collating reams of data on vaccinations, the US has counted too many shots as first doses when they are instead second doses or booster shots.” Here’s the tell: CDC data show 240MM people with at least one shot – about 72.5% of the population. But it also says only 203MM have been fully vaccinated, or 61.3%, an 11-percentage-point difference that is far larger than in other developed countries. So, either Americans are so lazy – or perhaps don’t want to endure another series of adverse reactions – that they won’t show up to get their second dose, or there’s something wrong with these numbers.
And it might not surprise you to learn that a number of state and local officials believes it’s the latter. “State and local officials say it’s improbable that 37MM Americans got one shot without completing their inoculations. Instead, they say, the government has regularly and incorrectly counted booster shots and second doses as first doses.” Their conclusion is that both fully vaccinated and completely unvaccinated are officially undercounted. As for the precise number miscounted, that’s unknown, but revisions in data from three states – Illinois, Pennsylvania and West Virginia – found enough over-counting of first shots to suggest that there are plenty of unvaccinated people nationally who’ve mistakenly been counted as having received a dose.
One of the biggest gaps identified was in Pennsylvania, where CDC estimates of first doses for the elderly exceed the state of Pennsylvania’s estimate by about 850,000. If changes are made to the national data on the scale of Pennsylvania’s revisions, this would mean increasing the number of Americans who are unvaccinated by more than 10MM. “The truth is, we have no idea,” said Clay Marsh, West Virginia’s Covid czar.
A resident doctor on CNN told viewers Thursday that they should all be wearing masks at home around other family members and everyone should wake up on Christmas morning and rather than open presents, take COVID tests. Dr. William Schaffner also said that these restrictions should apply to everyone, even those people who are double and triple vaccinated. “I recommend that we hang our stockings with care,” Schaffner stated, adding “We have to be careful because we are all going to get together, we should all be vaccinated and preferentially boosted. We should wear our masks if we are uncertain.”
“Another thing we could do is we could all get tested the morning of our getting together,” Schaffner further urged, before sharing a heartwarming story of how his own family did that for Thanksgiving. “We were all negative. It worked out just fine,” the doctor declared. Earlier in the year, Schaffner took to CNN to express his horror at Americans having fun at football games, complaining that they were “breathing too vigorously.” Schaffner declared “People are cheering and enthusiastic, exhaling with vigor; if there are people infected, they can infect people around them … Nobody was wearing a mask … I’d be very surprised if we didn’t have outbreaks.”
So where did the idea of "vaccine hesitancy" come from? The same people who are demanding you be vaxxed or else. SAME PEOPLE. pic.twitter.com/LgMf6eqC3C
CDC lists at least 3 conventional type vaccines (inactivated/killed virus as opposed to RNA/DNA) on its own website that are recognized by the United States government as producing immunity to COVID, yet no conventional vaccine is available in the United States. Why @CDCDirector? pic.twitter.com/WRDePjUbb1
South Africa delivered some positive news on the omicron coronavirus variant on Friday, reporting a much lower rate of hospital admissions and signs that the wave of infections may be peaking. Only 1.7% of identified Covid-19 cases were admitted to hospital in the second week of infections in the fourth wave, compared with 19% in the same week of the third delta-driven wave, South African Health Minister Joe Phaahla said at a press conference. Health officials presented evidence that the strain may be milder, and that infections may already be peaking in the country’s most populous province, Gauteng. Still, new cases in that week of the current wave were more than 20,000 a day, compared with 4,400 in the same week of the third wave. That’s further evidence of omicron’s rapid transmissibility, which a number of other countries, such as the U.K., are also now experiencing.
South Africa, which announced the discovery of the variant on Nov. 25, is being watched as a harbinger of what may happen with omicron elsewhere. Scientists have cautioned that other nations may have a different experience to South Africa as the country’s population is young compared with developed nations. Between 70% and 80% of citizens may also have had a prior Covid-19 infection, according to antibody surveys, meaning they could have some level of protection. Currently there are about 7,600 people with Covid-19 in South African hospitals, about 40% of the peak in the second and third waves. Excess deaths, a measure of the number of deaths against a historical average, are just below 2,000 a week, an eighth of their previous peak.
Pfizer said Friday it was changing plans and testing three doses of its COVID-19 vaccine in babies and preschoolers after the usual two shots didn’t appear strong enough for some of the children. Pfizer announced the change after a preliminary analysis found 2- to 4-year-olds didn’t have as strong an immune response as expected to the very low-dose shots the company is testing in the youngest children. It’s disappointing news for families anxious to vaccinate their tots. Pfizer had expected data on how well the vaccines were working in children under 5 by year’s end, and it’s not clear how long the change will delay a final answer.
Pfizer and its partner BioNTech said if the three-dose study is successful, they plan to apply for emergency authorization sometime in the first half of 2022. A kid-sized version of Pfizer’s vaccine already is available for 5- to 11-year-olds, one that’s a third of the dose given to everyone else 12 and older. For children younger than 5, Pfizer is testing an even smaller dose, just 3 micrograms or a tenth of the adult dose. Researchers analyzed a subset of youngsters in the study a month after their second dose to see if the tots developed levels of virus-fighting antibodies that were similar to teens and young adults who get the regular shots. The very low-dose shots appeared to work in youngsters under age 2, who produced similar antibody levels.
But the immune response in 2- to 4-year-olds was lower than the study required, Pfizer vaccine research chief Kathrin Jansen said Friday in a call with investors. Rather than trying a higher-dose shot for the preschoolers, Pfizer decided to expand the study to evaluate three of the very low-dose shots in all the study participants — from 6 months up to age 5. That third shot will come at least two months after the youngsters’ second dose. No safety concerns have been spotted in the study, the companies said.
Accurate estimates of COVID vaccine-induced severe adverse event and death rates are critical for risk-benefit ratio analyses of vaccination and boosters against SARS-CoV-2 coronavirus in different age groups. However, existing surveillance studies are not designed to reliably estimate life-threatening event or vaccine-induced fatality rates (VFR). Here, regional variation in vaccination rates was used to predict all-cause mortality and non-COVID deaths in subsequent time periods using two independent, publicly available datasets from the US and Europe (month-and week-level resolutions, respectively). Vaccination correlated negatively with mortality 6-20 weeks post-injection, while vaccination predicted all-cause mortality 0-5 weeks post-injection in almost all age groups and with an age-related temporal pattern consistent with the US vaccine rollout.
Results from fitted regression slopes (p<0.05 FDR corrected) suggest a US national average VFR of 0.04% and higher VFR with age (VFR=0.004% in ages 0-17 increasing to 0.06% in ages >75 years), and 146K to 187K vaccine-associated US deaths between February and August, 2021. Notably, adult vaccination increased ulterior mortality of unvaccinated young (<18, US; <15, Europe). Comparing our estimate with the CDC-reported VFR (0.002%) suggests VAERS deaths are underreported by a factor of 20, consistent with known VAERS under-ascertainment bias. Comparing our age-stratified VFRs with published age-stratified coronavirus infection fatality rates (IFR) suggests the risks of COVID vaccines and boosters outweigh the benefits in children, young adults and older adults with low occupational risk or previous coronavirus exposure. We discuss implications for public health policies related to boosters, school and workplace mandates, and the urgent need to identify, develop and disseminate diagnostics and treatments for life-altering vaccine injuries.
“Not only do the three vaccines authorized for emergency use require boosters due to waning “protective efficacy,” but they haven’t stopped breakthrough infections..”
Federal officials and advisors who have consistently boosted COVID-19 vaccines are starting to sound more like skeptics of the vaccines’ efficacy and safety. The face of the Biden administration’s COVID response is now making the same claims about vaccines that got a contrarian journalist booted from Twitter, while the CDC encouraged Americans to avoid a specific vaccine. National Institute of Allergy and Infectious Diseases Director Anthony Fauci cowrote a “perspective” in the New England Journal of Medicine (NEJM) Wednesday that acknowledged COVID vaccines were not living up to expectations. Not only do the three vaccines authorized for emergency use require boosters due to waning “protective efficacy,” but they haven’t stopped breakthrough infections, “allowing subsequent transmission to other people even when the vaccine prevents severe and fatal disease.”
Former New York Times reporter Alex Berenson wrote of the vaccines in August: “It doesn’t stop infection. Or transmission.” They have a “limited window of efficacy and terrible side effect profile.” Twitter permanently suspended him the same day for “repeated violations of our COVID-19 misinformation rules.” The social media company didn’t respond to Just the News queries seeking its distinction between claims by Berenson and Fauci and whether it would apply an “unsafe” warning to the NEJM essay, as it recently did to a study on increased heart risks in vaccine recipients, or otherwise restrict the publisher’s account. Twitter quietly updated its “COVID-19 misleading information policy” page sometime after Dec. 2, even while claiming through Wednesday that the update was made in November. (It corrected the month on Thursday, several days after Reclaim the Net noted the discrepancy.)
Among the new authority it grants itself, Twitter will punish users who claim vaccines, regardless of their authorization status, are “experimental”; taking them “would be more harmful than getting COVID-19”; and most pertinent to Fauci’s essay, vaccinated people “can spread or shed the virus … to unvaccinated people.”
“American doctors have proven to be cowards, cravens, zombies, and fools facilitating Dr. Fauci’s evil campaign — in concert with the rapacious pharmaceutical industry and a government in thrall to sinister forces that seek to destroy the country.”
The public health bureaucrat who styles himself as “the Science” is at it again. In his quest to eliminate the control group for his experiment in hazardous mRNA injections, Dr. Anthony Fauci reiterated his warning that the nation faces “a crisis of the unvaccinated.” Omicron is upon us, he told a US Chamber of Commerce meet-up this week, and the hospitals will soon be overwhelmed by the unvaxxed. Oh really? In fact, the gravest threat to America’s public health is… Dr. Tony Fauci and his debauchery of medical science. This will surely come as a surprise to readers of The New York Times, who see in the two-year (so far) Covid-19 event a splendid opportunity to hasten the destruction of the US economy and our culture in order to consolidate their own power to coerce and control the population. Clear the offices! Shut down the social spaces! Make ordinary business as difficult as possible! Cancel Christmas! That’ll git’er done!
In fact, Dr. Fauci is likely responsible for a preponderance of the total 802,000 US Covid deaths — putting aside the number of people who actually died from highway accidents, cancer, diabetes, old age, and other causes, but were listed as covid deaths by hospital accounting personnel avid for federal subsidy cash. It was Dr. Fauci who organized the suppression of easily marshaled and inexpensive early treatments for the disease, namely hydroxychloroquine, ivermectin, fluvoxamine, budesonide, azithromycin, monoclonal antibodies, Vitamin D, etc. It was Dr. Fauci who promoted the protocol of sending sick patients home from the ER without any treatment to await the further development of fatal clotting in their lungs. It was Dr. Fauci who designated the drug remdesivir — which he developed years ago for hepatitis-C (it did not work) with a financial stake in the patents — as the primary inpatient treatment for Covid-19.
And then it turned out that remdesivir destroys patients’ kidneys and is ineffective anyway in late treatment of the disease when viral loads wane and spike proteins have already created the fatal capillary clots in the alveoli of the lungs and in other organs. It’s Dr. Fauci who is responsible for the emergency use authorization on the mRNA “vaccines” that may have killed hundreds of thousands more Americans — based on the CDC’s VAERS system and statistical analysis of its inherent under-reporting at only 2.2 percent of all actual events— and you can add multiples more in non-fatal adverse reactions, including permanent disabilities. It’s Dr. Fauci who finagled the inadequate and botched trials of the mRNA vaccines in order to rush them into use.
And now it’s Dr. Fauci who wants to vaxx up all the children in America, despite evidence that the mRNA shots permanently disable children’s innate natural immune systems and can cause lasting heart, blood vessel, brain, and reproductive damage, and also despite the fact that few children are susceptible to serious Covid illness in the first place. [..] American doctors have proven to be cowards, cravens, zombies, and fools facilitating Dr. Fauci’s evil campaign — in concert with the rapacious pharmaceutical industry and a government in thrall to sinister forces that seek to destroy the country. The doctors have disgraced and dishonored themselves. The doctors have probably undermined their own vocations, as well as the entire armature of US health care, which they have allowed to become history’s worst racketeering operation.
“How carefully would you drive if it was mandated by law that you must have a 6″ spike mounted in the center of the steering wheel pointed at your chest — and seat belts were illegal?”
Folks, can we cut the bull**** please? Insurance companies are regulated. They are only permitted to make a certain amount of gross margin, typically 10%. Said regulation is enforced; firms are required to file their rates with state regulators along with the previous year’s results and projections for next. This applies to health insurance, car insurance, homeowners insurance, all insurance. Therefore there are exactly two ways for an insurance company to grow in size and profits: • Have more-frequent events results in a loss. • Have the same number of events but make them more expensive. That’s it. Efficiency is backwards because if you have overhead of 30% and cut it to 20% you don’t get to keep the other 10% in the company as profit which in any other line of business is yours to pocket. You wind up having to cut rates!
I have some data for health rates for firms in the midsized corporate world. I also have the Obamacare numbers for 2021 in a number of places, since those are published. They’re up. A lot. In some cases and places, by 30%. Do you really think the health insurance and health care providers care if you get a bad reaction from the jabs? No, they like it, provided it doesn’t kill you immediately. See the above for why. That you get ****ed is just business. You think the car insurance companies push all that expensive tech and “improvements” because it results in fewer crashes? Well, has it resulted in fewer crashes? Notice how the media and car companies, along with the insurance firms and their public-facing folks such as the crash-test people, always talk about fatality rates, not crashes.
A fatal car crash means you are no longer a customer. But that collapsible steering column isn’t for you, really — it doesn’t do anything to prevent the crash, it just costs more money if you crash and increases the odds you’ll live. This means (1) you’re still a customer and (2) the car costs more to repair or must be replaced. Obviously if you’re dead you don’t need another car, do you? Nor will you ever buy car insurance again. Oh, you think this is fanciful BS? Uh, nope. How carefully would you drive if it was mandated by law that you must have a 6″ spike mounted in the center of the steering wheel pointed at your chest — and seat belts were illegal?
A federal appeals court on Friday night reinstated President Joe Biden’s COVID-19 vaccine mandate for private companies with more than 100 workers, reversing lower court rulings and setting up a likely showdown before the U.S. Supreme Court. A three-judge panel of the 6th U.S. Circuit Court of Appeals ruled 2-1 that the U.S. Occupational Safety and Health Administration had the authority to Impose the mandate due to take effect Jan. 4. “Given OSHA’s clear and exercised authority to regulate viruses, OSHA necessarily has the authority to regulate infectious diseases that are not unique to the workplace,” the court conckuddd in its majority opinion.
Within an hour of the decision, the small business group Job Creators Network filed an appeal to the high court, saying the appeals judges “irresponsibly upheld an illegal rule.” “This mandate adds an incredible burden on small business owners who are still suffering negative effects of the pandemic,” the group said. “This mandate will make it even harder for small business owners to find and keep employees.” The ruling came after several challenges from GOP-led states and conservative and business groups were consolidated before the Cincinnati-based 6th circuit. The decision was supported by one Democrat-appointed judge and one Republican appointee and opposed by the third judge, who was appointed by former President Donald Trump.
Arkansas Attorney General Leslie Rutledge told The Associated Press she would immediately appeal to the Supreme Court. “The Sixth Circuit’s decision is extremely disappointing for Arkansans because it will force them to get the shot or lose their jobs,” she said. South Carolina Attorney General Alan Wilson, tweeted he was confident the mandate would be blocked by the justices. “We will go immediately to the Supreme Court- the highest court in the land- to fight this unconstitutional and illegal mandate,” he said. “The law must be followed and federal abuse of power stopped.”
More and more businesses in recent days have walked back previous rules mandating COVID-19 vaccines as a condition for employment in a bid to keep workers. Earlier this week, Amtrak—a quasi-public corporation—became the latest to rescind its vaccine requirement amid concerns about staff shortages and cut service in January. In a memo sent to staff that was obtained by The Epoch Times, Amtrak CEO William Flynn said the company would do away with the mandate that would have given employees until Jan. 4 to get fully vaccinated or go on unpaid leave. About 500 out of more than 17,000 Amtrak workers remain unvaccinated, according to the memo. Still, the sudden loss of that many workers would have caused service disruptions, Flynn suggested, while noting that Amtrak was acting in accordance with recent court orders handed down against President Joe Biden’s sweeping vaccine mandates.
Several hospitals and healthcare systems have similarly rescinded vaccine mandates for employees and cited labor issues that were triggered by the new requirements. In early December, Florida’s AdventHealth announced the end of its vaccine requirement for some 83,000 workers, also citing the several recent court injunctions against federal mandates. “Due to recent decisions by the federal courts to block the [Centers for Medicare & Medicaid Services] vaccine mandate, we are suspending all vaccination requirements of our COVID-19 vaccination policy,” AdventHealth Chief Clinical Officer Neil Finkler said in a letter to staff. The move came after the Centers for Medicare & Medicaid Services confirmed to The Epoch Times that the agency suspended enforcement following two court orders several weeks ago.
Tenet Healthcare, HCA Healthcare, and Cleveland Clinic recently announced they are pulling back as well, citing labor concerns. Along with AdventHealth, the three healthcare companies operate a combined 300 hospitals and have more than 500,000 workers. They cited recent court orders that blocked Centers for Medicare & Medicaid Services from enforcing its mandate on Medicare- and Medicaid-funded medical facilities. The rule was announced by Biden on the same day that he confirmed that he would impose mandates on federal government employees, businesses who have contracts with the federal government, and, most controversially, businesses that have 100 or more workers.
“Boeing has suspended its vaccine requirement in line with a federal court’s decision prohibiting the enforcement of the federal contractor executive order and a number of state laws.”
Boeing Friday said it has suspended its requirement that U.S.-based employees be fully vaccinated or face losing their jobs. The announcement comes as several attempts by President Joe Biden to require vaccinations for workers in various settings have been blocked by courts in recent weeks. “Boeing is committed to maintaining a safe working environment for our customers, and advancing the health and safety of our global workforce,” a company spokesperson told KOMO News. “As such, we continue to encourage our employees to get vaccinated and get a booster if they have not done so. Meanwhile, after careful review, Boeing has suspended its vaccine requirement in line with a federal court’s decision prohibiting the enforcement of the federal contractor executive order and a number of state laws.”
A U.S. District Court judge in Georgia on Dec. 7 issued a preliminary injunction against Biden’s executive order requiring all companies that contract with the federal government to have a vaccine mandate in place. The order was to have taken effect starting Jan. 4. Earlier orders requiring all employers with 100 or more employees to require vaccinations and one requiring all healthcare workers to be vaccinated have also been blocked by courts. Biden’s executive order requiring all federal workers to be vaccinated is facing 17 lawsuits, but no judges have granted requests to block it. Courts have also ruled that private employers, states, local municipalities and public universities are able to issue vaccine mandates.
In an internal memo to employees obtained by Defense News, Boeing said 92% of its U.S.-based workforce had either provided proof of vaccination or received a medical or religious exemption. “The success of Boeing’s vaccine requirement to date positions the company well to comply with the federal executive order should it be reinstated in the future,” the memo said. Reuters reported last month that some 11,000 Boeing employees, about 9% of its North American workforce, had requested an exemption. It is unclear how many were granted.
A “strict” Purple Ribbon outline will be applied immediately to all indoor shopping malls, the Prime Minister’s Office said late Friday night. The announcement came after two days of discussion on how to handle shopping malls, and as the number of coronavirus cases spikes across Israel. The decision was made jointly by Prime Minister Naftali Bennett, Health Minister Nitzan Horowitz, Economy Minister Orna Barbivai and MK Abir Kara. One person for every 15 square meters will be allowed to shop. And increased enforcement of mask wearing will be established. Moreover, the officials agreed, mall hours will be extended in order to accommodate shoppers and immunization complexes will be established in 50 main centers in the malls to encourage people to get the jab. Those who are vaccinated will enjoy special privileges.
Bennett had wanted to require the malls operate under the Green Pass outline, meaning that individuals would have to be fully vaccinated or take a COVID test to enter the facilities. The only exception would have been to access essential products. But fierce opposition by retailers and some members of the government on Thursday pushed the plan to the side. Friday night’s announcement said that if morbidity rates continue to climb then the Green Pass outline will once again be considered for any facility over 100 square meters. The above plan is still not final. It will be discussed at the cabinet meeting on Sunday, drafted as regulations and then voted on by the coronavirus cabinet via telephone poll. Once passed, the outline will begin immediately. Bennett is also reportedly expected to bring a resolution to the meeting that would mean almost the complete closure of the skies. Bennett’s proposal, N12 reported, is expected to include a ban on travel to most countries in the world, including the United States and other countries in Western Europe.
The development of polyvalent vaccines and new antivirals should lessen the need for social restrictions from around the middle of 2023, England’s chief medical officer has told MPs. Giving evidence to the House of Commons Health and Social Care Committee on 16 December, Chris Whitty said that although the UK may need intermittent social restrictions against covid-19 over the next 18 months, future medical advances should provide the “heavy lifting” against new variants. He said, “If I project forward, I would anticipate in a number of years, possibly 18 months, possibly slightly less, possibly slightly more, we will have polyvalent vaccines which will cover a much wider range [of variants].
And we will probably have several antivirals . . . and a variety of other countermeasures that mean that the great majority, and probably almost all, of the heavy lifting when we get a new variant—unless it is extremely different—can be met by medical means.” He added, “So I don’t see this as a kind of ‘we’re going to have to do this [social restrictions] repeatedly every few months’ situation. I think the risks will gradually decrease over time; it’s incremental.” However, Whitty said that for now some social restrictions may be necessary to tackle variants such as omicron that show some partial escape from vaccines and could overwhelm the NHS if left unchecked.
He said, “We’ve come from a place where we had absolutely nothing [in terms of medical interventions], so everything had to be done by social distancing and all the disruptive things that went with that right at the beginning. Where we are at the moment is kind of in a transition period. A very large amount of it can be done by [vaccines], and this is why the boosters are so absolutely essential, but we’re not quite in the rather safer haven I expect we will have in a couple of years’ time.”
A new covid-19 lockdown imposed last week (Dec. 7) in the port city of Ningbo, China, is raising the specter of further disruptions to an already battered global supply chain. There are more than 200 cases so far in the most recent cluster in the manufacturing province of Zhejiang, which includes the city of Ningbo. The outbreak is said to be spreading “relatively rapidly,” and has led to the closures of dozens of factories. So far, the lockdowns have restricted trucks going in and out of the port, slowing operations. While there are no reports yet of the port closing, the lockdown, combined with weeks of intensifying covid-zero restrictions, is worrying logistics professionals.
“The rising covid infections may lead to shutdowns at Ningbo and some other ports in China, adding to congestion and cargo backlogs,” a source from a UK-based logistics company said on Dec. 7 to S&P Global Platts, an analytics firm. “This is only the beginning—the first quarter of 2022 is going to be a complete wreck.” China’s pursuit of covid-zero has led to swift, severe measures to control the spread of infection, and policies to contain covid have only intensified since the omicron variant began to spread. On Monday (Dec. 13), Xinhua, the state-run news agency, singled out ports as the entry point for the most recent cluster of infections, and reported that the government will be tightening covid controls at port cities.
China’s policies at port have an outsized impact on the overall functioning of the global supply chain. The country is the world’s largest exporter of goods, as well as the largest importer of commodities. More ships call into the ports of China than any other country. “The global supply chain recovery relies on China,” said Atul Vashistha, CEO of Supply Wisdom, a New York-based risk intelligence company. “That’s an alarming and troubling truth considering China’s centricity to the supply chain. While it may be a sound public health policy, China’s zero-tolerance covid policy makes supply chain matters worse.”
”In May, Russia’s Ministry of Industry and Trade invited the Tesla CEO to discuss the possibility of opening a factory in the country, after he indicated that he was considering such a move.”
Russian President Vladimir Putin and South African-born billionaire Elon Musk could have a long-awaited meeting if the world’s richest man steps up and develops business interests in the country, the Kremlin has indicated. Speaking to journalists on Friday, Putin’s press secretary, Dmitry Peskov, said that the president has always been interested in meeting with foreigners who are keen to invest in Russia, adding that this could include Musk. “Without a doubt, the president is open to discussions with foreign businessmen,” Peskov explained. “There are regular discussions, practically every year, with French entrepreneurs, Germans, those with a large presence in our market. You and I know that Elon Musk isn’t in our market, but we hope that with time, he will become interested in it. And then, a meeting with the president isn’t out of the question.”
In February, Musk tweeted an invitation to Putin to chat with him via the audio-only social media app Clubhouse, writing, “It would be a great honor to talk with you.” The Kremlin replied that Musk’s invitation was “interesting,” and media reported that Putin hadn’t ruled out the possibility of a conversation. However, the meeting has not yet taken place. In May, Russia’s Ministry of Industry and Trade invited the Tesla CEO to discuss the possibility of opening a factory in the country, after he indicated that he was considering such a move. In addition to heading Tesla, the world’s most valuable automaker, Musk is also the founder of space transportation company SpaceX. In October, Forbes estimated his net worth at $271.3 billion, making him the richest person alive and, according to some measures, the richest in history.
From home confinement, Steven Donziger (@SDonziger) joined the #FreeAssange livestream event to show solidarity with fellow political prisoner.
Assange "represents ability to take on entrenched interests in our society, be they national security state" or fossil fuel industry pic.twitter.com/9cd6VNma2l
It is scary to see that the only thing that holds our societies together at this point is fear.
People can no longer think.
• In the entire world there are still no deaths reported from Omicron
• US: 110 total Omicron infections (UK has more)
• 1 person in US infected with Omicron hospitalized (may well be for something different)
But: UK prediction from scientists at the London School of Hygiene & Tropical Medicine:
• Best case: 175,000 hospital admissions and 24,700 deaths from Omicron by the end of April.
• Worst case: 74,800 deaths and 492,000 hospital admissions
“Pfizer Jab Is Only 22.5% Effective Against Omicron”: South Africa study.
So obviously the UK wants 1 million jabs per day. And Fauci wants more.
Two top soccer players, Napoli midfielder Piotr Zielinski and Man United defender Viktor Lindelof both left their game Sunday due to chest pain/breathing problems.
Ardern fund
WATCH: New Zealand PM Jacinda Ardern says her country has created a special account to fund journalists who will produce government-approved stories on Covid-19.pic.twitter.com/GkIFGsJkSD
The data are clear. Officials have reported110 Omicron cases as of Saturday in the USA. Of the 66 people for whom vaccination status has been reported, 52 were fully vaccinated and many of those had been boosted. What we don’t know is whether or not those people who have already had COVID-19 actually caught Omicron, but it was so mild that they weren’t aware of it or if prior infection conferred complete immunity. What we do know is that 78% of the people in the USA/CDC report who have contracted Omicron were vaccinated. These data also directly contradict the public relations “data” press release from Pfizer that the third jab would protect against Omicron. Clinical data ALWAYS trumps lab test data.
This appears to be yet another case illustrating that Fauci/Biden parrot the Big Pharma narrative whenever possible rather than doing the job that we are paying them to do – independently analyze “The Science” and act with integrity and objectivity to protect American citizens rather than American Big Business and Big Investment firms. There have been NO DEATHS reported anywhere in the world with Omicron, including in the USA. Now there will be, because older people, people with high co-morbidities will catch Omicron and will die. People die from the common cold too. We can expect this – do not be swayed by the fear-porn that is sure to come when these deaths happen. Hospital rates in areas with a high percent of the Omicron variant are experiencing a drop off in hospitalizations. Due to low vaccination rates in some countries, this strongly implies that vaccination status is irrelevant with Omicron. Omicron is a more mild disease, more similar in symptoms to the common cold. [..] Assuming that Omicron is now the dominant variant in Botswana, lets look at the death rate in that country: It has literally gone to zero over the past month.
Omicron is 10 times more infectious than the original variant and two times more infectious than Delta. Omicron will become the predominant strain in the USA very shortly. So, whether vaccinated or not, Omicron is more mild and will spread throughout the land. Let me write that again, all evidence shows that Omicron is much more mild and vaccinated or unvaccinated will catch this variant. Now, let’s talk children. For all the reasons listed above, it is clear that vaccinating children now is a very bad idea. 146 million people in the USA have had SARS-CoV-2 , that is about 45% of the total population. This means 45% of children have had SARS-CoV-2, that is the virus – because children rarely get severe disease from the virus. It is the severe disease that is COVID-19. COVID-19 is the severe disease caused by the virus. Historically, children get infected by the virus.
Now that Omicron will become dominant very quickly and we know that there is a very good chance that natural infection confers better protection against Omicron and that for everyone this new variant is mild, why would we want to mandate vaccination for our healthy children? Remember, this is what we know already before Omicron emerged: • 1 in 2700 male adolescents will get pericarditis/myocarditis from the Pfizer vaccine and the event rate appears to be even higher for Moderna. • 1 in 2200 will get some sort of neurological event from the vaccine (based on the curious case of Pfizer clinical trial participant Maddie de Gary). • That the adverse events in children are much higher than originally reported in the phase 3 clinical trials. • That the long term sides effects for this vaccine are unknown. • That after vaccination, there is a 3-4 week period of immunosuppression, where children (and adults) are susceptible to latent viral infections and other viruses.
Now smash these facts together with what we know about Omicron. The evidence becomes overwhelming. Not only are mandates a bad idea, but vaccinating children and young adults is too. This is madness promoted by frightened psychotic chickens and Globalists with a pro-totalitarian bias. Just stop. Now.
Two competing forces will determine Omicron’s impact on the nation over the next few weeks. The power of booster jabs to give last-minute protection against Covid-19 will be pitted against the new variant’s ability to elude existing immunity. The outcome will decide whether our festive season is going to be muted or miserable. If enough arms are jabbed with booster vaccines, while Omicron turns out to have poor powers to evade immunity, then there is hope hospital cases will be contained and the NHS will be protected. Severe restrictions in the new year – including the prospect of lockdowns – could be avoided. But if Omicron is found to evade existing immunity quite easily, while booster campaigns provide poor overall protection, then the country faces a very grim winter with strict restrictions needed for some time.
According to a study by scientists at the London School of Hygiene & Tropical Medicine, the first scenario – poor Omicron escape from immunity matched by effective booster jab protection – would trigger a wave of infection that could lead to 175,000 hospital admissions and 24,700 deaths by the end of April. Closure of some entertainment venues and restrictions on indoor hospitality would be enough to control case numbers. By contrast, the most pessimistic scenario – high immune escape from vaccines and low effectiveness of booster jabs – would see 74,800 deaths while there would be 492,000 hospital admissions, a figure twice as high as the peak seen in January 2021. Far stricter restrictions, including lockdowns, would then have to be considered.
“These results suggest that Omicron has the potential to cause substantial surges in cases, hospital admissions and deaths in populations with high levels of immunity, including England,” the team state in their paper, which has not yet been peer-reviewed. Nicholas Davies, co-leader of the study team, described Omicron’s threat to the UK as “worrying”. Presented with evidence like this, many scientists have warned that urgent action should now be taken to hold back infections while booster campaigns are accelerated and given time to take effect. “Cases are doubling every two to three days which means there is a real risk the curve is going to get very steep around Christmas and New Year,” said the vaccine expert Peter English.
“That means panic measures could be brought in at the last minute and disrupt people’s festive plans. I am also desperately sad for my colleagues in clinical practice who face a January that is going to be worse than anything we’ve seen so far and at a time when they are now exhausted.”
Boris Johnson is gambling on an unprecedented ramping up of vaccinations, rolling out 1m booster jabs a day to stem an incoming “tidal wave of Omicron” and avoid imposing further restrictions. The army will be deployed across the country to help rapidly accelerate the vaccine programme and GPs will be told to cancel appointments to dedicate resources to offering vaccines to every UK adult by the end of December. In a televised address to the nation on Sunday night, the prime minister said he was “afraid we are now facing an emergency in our battle with the new variant, Omicron, and we must urgently reinforce our wall of vaccine protection to keep our friends and loved ones safe.”
Johnson, who is facing a major test of his authority this week as MPs rebel against new Covid restrictions, called the target “a national mission unlike anything we have done before in the vaccination programme”. It means vaccinating around 1 million people a day, up from 530,000 on Saturday. The UK record is 844,000 in March. All over-18s will be eligible from Monday, and NHS booking will open to that age group from Wednesday. Until now eligibility has been limited to over-40s. Jabs will be available on Christmas Day, though demand is expected to be low.
On Sunday the Covid alert level was raised from 3 to 4, indicating substantial pressure on the NHS, after a further 1,239 UK cases of Omicron were confirmed, nearly double the number reported the previous day. Omicron is expected to become Britain’s dominant variant within days, and Johnson warned it could “overwhelm the NHS and lead to very many deaths”. Announcing the booster offensive, Johnson said: “We know from bitter experience how these exponential curves develop. No one should be in any doubt: there is a tidal wave of Omicron coming.” He said two doses of vaccine were not enough, but scientists were confident that three would make a huge difference. On Friday UK data suggested that three jabs provide 70-75% protection against infection with Omicron, while two doses given three or more months ago give 30% to 40% or less.
A few days ago, researchers in South Africa shared data from a preliminary study showing that the Pfizer vaccine is less effective at blocking the omicron variant than earlier variants like beta and delta. Now, the team is telling us exactly how much less effective the vaccine is. According to the same data gleaned from the blood plasma taken from 12 patients who tested positive for omicron, the team found that a two-shot course of Pfizer’s vaccine has just 22.5% efficacy against symptomatic infection with the omicron variant, though it can thwart severe disease, according to laboratory experiments in South Africa, according to Bloomberg.
The data comes courtesy of a team of researchers at the Africa Health Research Institute in Durban. Though data has been pouring out about omicron, and sometimes individual studies reach opposing findings, the general consensus is that omicron will be able to more easily evade protection afforded from the first generation of vaccines – however, the scientists say that people will still be protected against severe disease and death. But it matters less anyway, since any patient – even an unvaccinated one – has less to fear from omicron. The reason being is that it’s believed to cause a more mild, “flu-like” infection. As we’ve said before, when you hear politicians like Joe Biden talking about an omicron takeover as if it were already a certainty (only a couple thousand cases have been confirmed around the world, if that), it’s because they wish it were true.
The same is true for the CEOs of Moderna and Pfizer, who have been out sharing FUD about omicron with the news media on an almost non-stop rotation. They say their companies can have a new batch of vaccines available in 90-100 days. It’s almost as if they’ve been waiting for the opportunity, and if you look back at their comments, it’s clear that they have. Still, in the US, the CDC has confirmed that only 1 of 43 patients infected with the variant has been hospitalized.
National Institute of Allergy and Infectious Diseases director Dr. Anthony Fauci said that Americans will “just have to deal with” the prospect of getting more coronavirus booster shots. Fauci made the statement on Sunday morning and said that the level of protection that the current coronavirus booster shots give to individuals will have to be monitored closely over the next several months. “If it becomes necessary to get yet another boost, then we’ll just have to deal with it when that occurs,” Fauci said. The National Institute of Allergy and Infectious Diseases director also said that he’s “hoping” that a third mRNA shot will give longer-lasting protection. “
I’m hoping from an immunological standpoint that that third shot of an mRNA and the second shot of a J&J will give a much greater durability of protection than just the six months or so that we’re seeing right now,” Dr. Fauci said. He added that it’s possible that the booster shot could “dramatically” increase the level of protection. “It’s tough to tell because the third shot of an mRNA could not only do what we absolutely know it does, is it dramatically increased the level of protection. But from an immunological standpoint, it could very well increase the durability of protection by things that you can’t readily measure by the level of antibodies that you might have a maturation of the immune system that would prolong the durability,” Dr. Fauci said.
Early on in the pandemic, before the vaccines were available, the Southern Brazilian city of Itajai offered Ivermectin as a prophylaxis against the disease. Between July and December of 2020, roughly 220,000 people were offered a dose of 0.2mg/kg/day (roughly 18mg for a 200lb person) as an optional treatment for 2 days, once every two weeks. 133,051 people took them up on it, while 87,466 did not. After analyzing the data, a team of researchers spanning several Brazilian institutes, the University of Toronto, and Columbia’s EAFIT concluded in a December pre-print study that hospitalization and mortality rates were cut in half over the seven month period among the Ivermectin group.
This is even more impressive when you learn the IVM users were older on average, with 30% >50 yo versus 20% for non-IVM users. The mortality reduction is even higher looking at different age groups. 85% for 31-49 yo and 59% for >50 yo. pic.twitter.com/K6D5naybCS
The authors adjusted for relevant confounding variables, including age, sex, medical history, previous diseases, and other conditions. The analysis contradicts an October report by Business Insider which claims, based on a Brazilian ICU doctor’s anecdotal evidence, that the experiment was a failure. Study limitations: The authors note, “Being a retrospective observational analysis, it is uncertain whether results would be reproducible in a randomized, placebo-controlled, double-blind clinical trial, but likely, since groups of ivermectin users and non-users had similar demographic characteristics, and rates were adjusted for the relevant confounding variables.”
We’re sure the ‘fact checkers’ are already hard at work trying to debunk the pre-print, however they may also want to take a look at ivmmeta.com – a real-time meta analysis of 70 studies which found that Ivermectin works as a prophylaxis 83% of the time. In peer-reviewed studies, it was found effective 70% of the time as an early treatment, and just 39% of the time as a late treatment. As we noted during the whole ‘horse paste’ controversy: Ivermectin This widely prescribed anti-parasitic which is also used in horses has shown meaningful efficacy worldwide in the treatment of mild and moderate cases of Covid-19, plus as a prophylactic. India’s Uttar Pradesh province, with a population of over 200 million, says that widespread early use of Ivermectin ‘helped keep positivity [and] deaths low.’
Gerald Celente, a renowned trends researcher, is back this time to talk about what he is sees coming in 2022. There is the never ending Covid, Vax Wars, military wars, economic upheaval, and even new predictions on the future of Donald Trump, Hillary Clinton and Ron DeSantis. We start with what needs to be done to defeat the tyranny of the vax war on the global population. Celente says, “Vax War,’ look at the protests going on in Austria. Look at the protests going on in Germany, Italy, in France and the UK. . . . The only way this war will be won is if people unify under one umbrella and don’t leave.”
On the economy, Celente warns, “How about that bankster, that Fed Head Powell? He said inflation was going to be ‘temporary.’ Oh no, it’s going to be ‘transitory.’ They were shooting out that BS one after another, and we said from the beginning, inflation is real and it’s going to keep going. Guess what? It’s not the supply chains–it’s all the cheap money they keep dumping into the system to artificially prop it up.” Celente predicts, “The Fed is going to have to raise interest rates,” to stop what he is calling 1980’s style inflation. And he warns, “The higher interest rates go up, the further the economy is going to go down, and that’s what they are not talking about.”
Celente says get ready for what he is calling “Dragflation.” Meaning, the economy is going to drag lower as inflation surges higher. Celente also predicts that if the Fed Funds Interest Rate, which is now at .25%, “goes to 1.5%, the entire economy could collapse.” Celente is predicting new political parties that are anti-immigration and anti-establishment to form next year. Celente also gives what his assessment of Donald J. Trump, Hillary Clinton and Ron DeSantis are for the year 2022 and beyond. Celente also makes a bold prediction on the so-called CV19 mandates that should make the unvaxed feel more secure. The negative effects of vaccines are going to stay in the news, but Celente expects the mainstream media (MSM) to do everything possible to cover up the deaths and injuries caused by the CV19 injections. Will the numbers be overpowering to the MSM?
Four states – Indiana, Maine, New Hampshire and New York – are deploying the National Guard to battle the COVID-19 healthcare staffing shortage. The staffing shortage rose sharply following the implementation of a vaccine mandate. Vaccination rates in New York, New Hampshire and Maine are some of the highest in the nation. More than 80% of people in these states have received at least one dose. In New York, thousands of healthcare workers were placed on unpaid leave after refusing to get the shot. The Guard, under the direction of Gov. Kathy Hochul (D) will send about 120 medical workers to 12 long-term care facilities, according to the Epoch Times. About 75 Guard members from Maine were deployed by Gov. Janet Mills (D). Over the past week, the largest hospital in Maine has not had any available critical care beds.
The New York Times reports that cases in Maine reached their pandemic peak recently. In New Hampshire, about 70 National Guard members are providing medical support across the state. “If unfortunately during the winter months, the hospitalization rates continue to increase, we’ll be more than happy to provide additional resources,” National Guard Maj. Gen. David Mikolaities said according to Epoch Times. Indiana called in the Guard last week to 13 facilities throughout the state following a request from Indiana University Health. The facility fired about 125 people who refused to comply with the school’s COVID-19 vaccine mandate. The Hoosier State has a vaccination rate of 56.7 percent of residents having received at least one dose.
Maine
Hospitalizations in Maine are up 902% since July, even with 99.9% of seniors at least partially vaccinated and 63% having had a booster shot
Who would have guessed that unmasked and unvaccinated college football fans in the South could do this to them? pic.twitter.com/FHjg504vXz
In a stunning admission, virologist Dr. Andrew Hill acknowledged in a zoom call that publication of his study could lead to the deaths of at least a half million people. In defending his reversal on the effectiveness of ivermectin as a treatment for COVID-19, he discussed his “difficult situation” and said, “I’ve got this role where I’m supposed to produce this paper and we’re in a very difficult, delicate balance.” The incident is recounted in Robert Kennedy Jr’s New York Times Bestseller, The Real Anthony Fauci: Bill Gates, Big Pharma, and the global war on Democracy and Public Health. Andrew Hill, PhD, is a senior visiting Research Fellow in Pharmacology at Liverpool University. He is also an advisor for the Bill and Melinda Gates Foundation and the Clinton Foundation.
As a researcher for the WHO evaluating ivermectin, Hill wielded enormous influence over international guidance for the drug’s use. Hill had previously authored a analysis of ivermectin as a treatment for COVID-19 that found the drug overwhelmingly effective. On Jan. 6 of 2021, Hill testified enthusiastically before the NIH COVID-19 Treatment Guidlelines Panel in support of ivermectin’s use. Within a month, however, Hill found himself in what he describes as a “tricky situation.” Under pressure from his funding sponsors, Hill then published an unfavorable study. Ironically, he used the same sources as in the original study. Only the conclusions had changed.
Shortly before he published, Dr. Tess Lawrie, Director of the Evidence-based Medicine Consultancy in Bath, England, and one of the world’s leading medical research analysts, contacted Hill via Zoom and recorded the call (transcript below). Lawrie had learned of his new position and reached out to try to rectify the situation. In a remarkable exchange, Hill admitted his manipulated study would likely delay the uptake of ivermectin in the UK and United States, but said he hoped his doing so would only set the lifesaving drug’s acceptance back by about “six weeks,” after which he was willing to give his support for its use. Hill affirmed that the rate of death at that time was 15,000 people per day. At the 80 percent recovery rate using the drug, which Hill and Lawrie discussed earlier in the call, the number of preventable deaths incurred by such a delay would be staggering — as many as 504,000.
Twitter has quietly updated its “COVID-19 misleading information policy” to impose new sanctions on tweets about vaccines, PCR tests, and health authorities. These sanctions include removing and labeling tweets. Both types of sanctions also result in Twitter users accruing strikes on their account which can lead to a permanent suspension. While the top of Twitter’s COVID-19 misleading information policy page currently states “Overview November 2021,” a December 2 archive of the page shows that the page was updated and the “Overview November 2021” text was added after December 2. One of the most notable changes to this “COVID-19 misleading information policy” we noticed is related to claims about whether vaccinated people can spread the coronavirus.
The policy now states that Twitter will label tweets with “corrective information” and give users a strike if they: • Claim that “the vaccines will cause you to be sick, spread the virus, or would be more harmful than getting COVID-19”. • Post what Twitter describes as “false or misleading claims that people who have received the vaccine can spread or shed the virus (or symptoms, or immunity) to unvaccinated people”. This means Twitter users could now be sanctioned for sharing or discussing the Centers for Disease Control and Prevention’s (CDC’s) admission that “vaccinated people can still become infected and have the potential to spread the virus to others.”
Another change is that Twitter will start giving a strike to and labeling the tweets of users that use research and statistical findings to “make claims contrary to health authorities,” if it decides that their claims “misrepresent research or statistical findings pertaining to the severity of the disease, prevalence of the virus, or effectiveness of widely accepted preventative measures, treatments, or vaccines.” Previously, Twitter would sanction what it deemed to be “false or misleading” information about research findings but there was no provision about contradicting health authorities.
In addition to this, Twitter will give users two strikes and remove their tweets if they claim that “vaccines approved by health agencies (such as Pfizer’s Comirnaty vaccine in the United States) did not actually receive full approval/authorization, and therefore that the vaccines are untested, ‘experimental’ or somehow unsafe.” This appears to be a reference to criticism of a footnote in the Federal Drug Administration (FDA’s) “full authorization” documents for the Pfizer-BioNTech (Comirnaty) vaccine which revealed that the FDA had extended the emergency-use authorization for the same vaccine. Furthermore, users that claim that vaccines are part of a “global surveillance” effort will have their tweets removed and be given two strikes. The introduction of this provision follows vaccine-related surveillance tech, such as vaccine passports, being introduced in many countries.
“China’s rapid industrialization and hunger for global market share kept deflationary pressure on durable goods prices for thirty years, helping to keep consumer price inflation and interest rates lower in the West. And the beauty of the Magic Money Tree was that China could insulate its highly cyclical industry from any default cycle. It monetized bad debt and preserved unprotected, deflationary capacity. The stock of money ballooned. Banking assets are now around $52 trillion. They’ve grown by about $40 trillion since 2008. They’re now twice the size of the US banking system and China’s banks have added the equivalent of the US banking systems in just eight years. This is what hyper MMT looks like.”
“The net result is that western monetary policy and China’s mercantile model fed off one another to give us this Alice in Wonderland ‘through-the-looking-glass’ transformation of massive monetary growth into a deflationary mechanism: The Refrigeration Mode. Both sides got what they wanted: China leapfrogging industrial development, and the US got low inflation in the great moderation. But it had side effects. A massive monetary overhang in China, hyper financialization in the US. These extremes are now biting back on the system through the political economy.” “The Deflationary D’s may still be with us (debt, demographics, disruption, digitization), but the system dynamic is becoming inflationary and there are some new supply side shocks that aren’t deflationary for a change.
“Both sides are in (re)flux. On the macro policy side, we are seeing powerful social reactions to the extremes produced by The Refrigeration Mode. These extremes are feeding into the political economy. Whether it’s the ‘Tax the Rich’ dress at the Met Gala, politicians and celebrities at climate change marches around the world, or bipartisan support for China containment, the challenge to the status quo is clear and present. The COVID crisis merely poured petrol on it.” “It means fiscal policy is back in the driver’s seat – just as central banks put an inflationary bias into their reaction functions. Future bailouts are coming via Main Street, as much as Wall Street. And when monetary and fiscal policy combine, policy becomes more directly inflationary in CPI terms, not simply in asset price terms.”
Rona the red spike protein
https://twitter.com/i/status/1469868738820386817
Vaccine Propaganda
Covid Vaccine Propaganda Exposed. Why did so many blindly get vaccinated without thinking? Popular culture, media, celebrities, politicians, athletes, social media creators, emotional appeals, & slogans. Spread fear, then offer the solution to freedom & getting your life back. pic.twitter.com/xK3fUhlfyE
The World Health Organization (WHO) has informed The Epoch Times that it has not documented any deaths from the Omicron variant of the CCP (Chinese Communist Party) virus, which causes COVID-19. According to the WHO, “for Omicron, we have not had any deaths reported, but it is still early in the clinical course of disease and this may change.” When reached for comment by The Epoch Times, the Centers for Disease Control and Prevention (CDC) sent its report on the Omicron variant in the United States from Dec. 1 through 8. It shows that there were no documented deaths from Omicron during that period. The WHO’s latest weekly epidemiological update for Dec. 7 showed that all 212 Omicron cases documented across eighteen European Union (EU) countries were either mild or asymptomatic.
“While South Africa saw an 82 percent increase in hospital admissions due to COVID-19 (from 502 to 912) during the week 28 November–4 December 2021, it is not yet known the proportion of these with the Omicron variant,” the report noted. Omicron has also been detected in the United States, first in California and later in Colorado, New York, Maryland, Utah, and many other states. The first American patient with the variant was identified in San Francisco, testing positive for COVID-19 on Nov. 29 after returning from a trip to South Africa on Nov. 22. Yet the California Department of Public Health has confirmed to the Los Angeles Times that the variant was present in wastewater as early as Nov. 25.
Note the subtle lower placement of the Fluzone data graphs, making the mRNA product appear more effective than it is relative to the licensed traditional Fluzone graphs. In a sharp-eyed tweet, @RobertLKruse gets the gold star for pointing out this trick in Moderna’s slide comparing early efficacy data from its flu shot to a competitor. The y-axis being lower for Fluzone’s shot is lower makes it look worse (and $MRNA’s shot better) if glancing quickly and comparing the two graphs. For some reason, Moderna seems to have failed to perform statistical comparison of Fluzone versus Moderna flu jab data. Perhaps because they do not have enough capital to hire competent biostatisticians to run the numbers?
Panel B: Safety – Adverse events
This is the real bombshell! Note that the dose for Moderna’s COVID-19 jab is 100 micrograms, so focus on that column when comparing to placebo- 92% of patients >= 50 years old had adverse events, compared to 33% in the placebo. Even in 18 – 50 year olds – who really have no reason to be vaccinated against COVID-19 with these products- the data show a 90.5% adverse event rate compared to 30% in placebo treated patients. This does not look good. What we can infer from this is that the adverse event profile for the mRNA COVID-19 jabs that has so many of us (including myself!) alarmed is not just due to the Spike protein, but a significant proportion of the risk seems to be due to the artificial pseudouridine-containing mRNA combined with the novel synthetic cationic lipid (positively charged synthetic fat carrier molecule).
Japan announces that public and private sectors can not discriminate against those who refuse the experimental mRNA gene therapy injections. Japan is now labeling Covid “vaccines” to warn of dangerous and potentially deadly side effects such as myocarditis. In addition, the country is reaffirming its commitment to adverse event reporting requirements to ensure all possible side effects are documented. These efforts from Japan’s health authority are in stark contrast to the deceptive measures taken by other countries to coerce citizens into taking the injection, downplaying side effects, and discouraging proper adverse event reporting. Additionally, Japan is emphasizing informed consent and bodily autonomy. Until the coronavirus pandemic, the concept of “informed consent” was considered sacred to healthcare professionals in the West.
Japan is particularly raising concerns about the risks of myocarditis in young men injected with Pfizer or Moderna’s gene–therapy treatment. The country is enforcing a strict legal reporting requirement of side effects that must take place within 28 days of the injections. Three Covid-19 gene-therapy treatments are currently offered in Japan. They include the Pfizer/BioNTech (Comirnaty) and Takeda’s Moderna formulation. The product descriptions state that “this product contains an additive that has never been used in a vaccine before.” Furthermore, the pharmaceutical companies urge you to consult your doctor about the additive if you plan to be injected with it. In addition to the Pfizer and Moderna gene-therapies, Vaxzevria (formerly AstraZeneca) is also administered in Japan. However, Japan only recommends it to people 40-year-old and over. Reference is also made to the new type of additive in the Vaxzevria injections.
Japan’s Ministry of Health of health website encourages citizens to receive the “vaccine”; however, they stress it is not mandatory, “Although we encourage all citizens to receive the COVID-19 vaccination, it is not compulsory or mandatory. Vaccination will be given only with the consent of the person to be vaccinated after the information provided.” In addition, the government recommends those who are considering taking the shot carefully consider both its effectiveness and side effects. “Please get vaccinated of your own decision, understanding both the effectiveness in preventing infectious diseases and the risk of side effects. No vaccination will be given without consent.” Furthermore, they stress that businesses do not force employees to receive the experimental gene therapy. Nor should employees discriminate against those who refuse the injections,
“These concerns are particularly acute in the case of children, who may well be exposed to the risk of very serious illness in the future, if vaccination permanently misdirects their immune system.”
The severity of Corona infection varies wildly across the population. Children have generally mild or asymptomatic infections, while adults having a wide range of responses. Everyone always assumed that cross-immunity was part of the answer to this conundrum. The problem, is that it is shaping up to be a not very reassuring part of that answer. The untrained, innate non-specific immune response of children looks more and more like a big part of the reason they are spared severe infection. Adults with immune systems tightly calibrated to the common human coronaviruses , meanwhile, often have more severe symptoms. They suffer from Original Antigenic Sin. Over 4.2 billion people across the earth have received at least one dose of vaccine against SARS-2.
The majority of these vaccines have elicited antibodies only against an early form of the spike protein that is no longer in circulation. This would seem to be one reason why many western countries with high vaccination rates appear to have locked themselves into an indefinite phase of heightened SARS-2 transmission. In the United Kingdom, 96% of adults have antibodies to the spike protein – most of these first acquired by vaccination. Shortly after they concluded their vaccination campaign, cases skyrocketed, and they have remained high ever since. Original Antigenic Sin is a real phenomenon. It seems not only to permanently influence the immune response to the spike protein itself, but also to inhibit the development of antibodies to other SARS-2 proteins.
A worst case scenario, would be a future spike mutation that entirely escapes the anti-spike antibodies elicited by our vaccines. In this case, it seems possible that many vaccinated people will be stuck with permanently suboptimal immune responses. If Omicron is indeed circulating primarily among the vaccinated, as some data shows, this would be a good reason why. These concerns are particularly acute in the case of children, who may well be exposed to the risk of very serious illness in the future, if vaccination permanently misdirects their immune system.
Frequent re-exposure solves the problem of a rapidly evolving virus by updating our immune system to recognize and neutralize closely related variants before we lose all our protective immunity from a previous infection. As long as the interval between exposures is not too long, you will still have cross-reactive immunity from your last exposure to protect you during your next “update”. Re-infection does not necessarily mean you will get sick. As long as it happens while you still have partial cross-reactive immunity, your “update” might be mild or you may not get any symptoms at all. In other words, we have to stop thinking of our immune systems as mere protective shields. They are much more than that.
We need to remind ourselves that our immune systems are self-improving protective shields that need frequent exercise in order to maintain and update their skillset to keep up with an evolving enemy. The propaganda during Covid has not denied this fact, it has merely distorted it to the point where many people have lost faith in their immune systems, have become terrified about every “variant of concern”, and have become fixated on vaccines as the only path to salvation. Fear doesn’t just blind us to what is standing before our eyes. It also makes us doubt our own senses and forget our long-established understanding of the world. Frequent re-exposure is nature’s solution to booster shots. Vaccine boosters make more sense for diseases in which re-exposure is so rare that immunity wears off entirely before you are likely to get a natural update.
It’s worth reminding ourselves that there are over 200 respiratory viruses that cause colds and flus and yet, despite the fact that they are permanently circulating in our communities, we do not get sick with dozens and dozens of colds and flus every year. Although we won’t be exposed to every single one of these 200 viruses every single year, we will cross paths with many of them. But as long as our immune systems have not been weakened by some serious pre-existing health condition (i.e. obesity, cancer, HIV, etc.) or by lifestyle choices that temporarily suppress our immune systems (i.e. poor sleep, lack of exercise, vitamin C or D deficiencies, stress, depression, isolation, etc.), most of these “updates” will merely be mild or asymptomatic infections because our immune systems encounter them so often.
At the end of August, a study was published showing that natural immunity provides much better protection against infection than the Pfizer vaccine. It was described by UCL’s Francois Balloux as “a bit of a bombshell”. Subsequent studies have compared natural and vaccine-induced immunity at the cellular level. One found that infection-induced antibodies “exhibited superior stability and cross-variant neutralisation breadth” than vaccine-induced antibodies, suggesting that people who’d already been infected had better immunity against the then-novel Delta variant. However, as I noted in my write-up of the “bombshell” study, its findings still needed to be replicated. After all, certain datasets or methods of analysis can sometimes yield quirky results, which don’t survive independent empirical tests.
Encouragingly, the findings now have been replicated – by another team of Israeli researchers, using a different dataset. In the latest study, Yair Goldberg and colleagues tracked all the individuals in their dataset (of people in Israel) who had tested positive or received two doses of the Pfizer vaccine before 1st July, 2021. They then compared the number of infections in previously infected versus vaccinated individuals from August to September of 2021. The researchers also examined the number of infections among those with so-called ‘hybrid immunity’ – i.e., previously infected individuals who got vaccinated. For each of the three groups, they counted the number of infections and the number of days ‘at risk’ (i.e., the total number of people multiplied by the number of days on which they were ‘at risk’ of becoming infected). Adjustments were made for age, sex, ethnicity, calendar week and a measure of risk exposure.
Results are shown in the chart below. Each bar corresponds to the infection rate per 100,000 ‘risk days’. The reason the researchers used ‘risk days’, rather than just ‘people’, is that the composition of each group changed over time. For example, some previously infected people chose to get vaccinated. Notice that the labels for the horizontal bars are not the same for each group. Since we want to compare apples with apples, look at the bars labelled “Recovered 6–8 months” and “Vaccinated 6–8 months”. This comparison shows that, 6–8 months after the corresponding event, infection rates were more than six times higher among vaccinated individuals – 89 per 100,000 versus only 14 per 100,000 among previously infected individuals.
“There are teachers who call children individually and ask them about their vaccination status: those who are vaccinated receive applause, those who do not have to justify themselves.”
“It seems as if it has been forgotten that the vulnerable group does not sit in kindergartens and schools.”
Hardly anything is discussed as emotionally as concerns about children in the pandemic. The reasons for this could not be more different, there is only consensus that almost all parents feel abandoned by politics. Although the previous plans of the traffic light parties no longer provide for nationwide school closings, regionally these will also be possible in the future. Conditions that include alternating and distance lessons as well as distance rules are not expressly excluded. In some federal states, compulsory attendance has already been lifted and the first schools have been closed again.Many parents are now ready to accept further measures if only the educational institutions remain open this winter. At the same time, scenes are playing out in schools that would have sparked an outcry from society before the pandemic. There are boards with the vaccinated on one side and the non-vaccinated on the other, who then have to undergo regular tests in front of the assembled class.
There are teachers who call children individually and ask them about their vaccination status: those who are vaccinated receive applause, those who do not have to justify themselves. Adolescents remind their classmates of their “social responsibility” by mistakenly assuming that it is they who have a responsibility for adult society, not for them. The social division has long since reached schools. This is certainly not the case in all schools, but unfortunately they are not isolated cases either. The medical benefit of the vaccination for 12 to 17-year-olds is given, but limited, as Stiko member Rüdiger von Kries recently emphasized in an interview with Bayerischer Rundfunk. Most young people are – and rightly so – not afraid of infection. Nevertheless, many would like to be vaccinated: because they want to live their youth, want to evade the pressure exerted on them and avoid the requirements that apply to those who have not been vaccinated.
The Standing Vaccination Commission (Stiko) generally recommends vaccinating children and adolescents from the age of 12 against Covid-19, but has explicitly opposed vaccination for children and adolescents to participate in education, culture and other social activities is made dependent. So it says in the recommendation. But politics, with its sometimes disproportionate measures against this age group, prevents their social participation. So 2G is spreading even further for this age group. Children and adolescents from 12 (or 16) years of age no longer have access to public facilities in many places, regardless of their negligibly low risk of developing a serious disease. Von Kries calls such an obligation “simply absurd”. And now that the European Medicines Agency (EMA) has approved the vaccine for children under the age of 12, it must be feared that the younger ones will face the same threat.
A fact-based classification on the basis of scientific evidence no longer seems possible. The parents’ trust in political decisions for the benefit of adolescents has been lost. It seems as if it has been forgotten that the vulnerable group does not sit in kindergartens and schools.
German kids
In Germany, children are being forced “to go to the front of the class and state their vaccination status daily. Those who are vaccinated are applauded, those who are not have to explain why they are not.”pic.twitter.com/k9nmI4Smx4
Google translate. Note the neat trick: much of the correspondence is done with text messages, like Whats App. Which are not archived (“by their nature short-lived”), and therefore don’t exist, officially. Handy when an FOIA request comes in. Click here for the uncensured 104-page contract.
The European Commission does not want to make possible agreements between Ursula von der Leyen and the pharmaceutical giant Pfizer transparent. This emerges from a response from the Commission to the EU ombudswoman Emily O’Reilly, which netzpolitik.org has now published. Specifically, it is about messages that the EU Commission President is said to have exchanged directly with Pfizer CEO Albert Bourla in order to thread a vaccine deal. The New York Times reported on the existence of the news in April. The deal involved 1.8 billion doses from Pfizer-BioNTech. The billion dollar deal for the vaccine was agreed this spring, when the great majority of Europeans were still unvaccinated, via the short official channel in calls and messages directly between Ursula von der Leyen and Albert Bourla, according to the report of the renowned US newspaper . The “text messages” referred to there can mean both SMS and messages via messengers such as Signal or WhatsApp.
Its vaccine Comirnaty makes the consortium of Pfizer and the German company BioNTech the most important vaccine supplier to the EU. But how it sets prices for its vaccines and which countries are preferred for delivery remains in the dark, according to an investigative research by the Financial Times. “How Pfizer is exercising its newfound power – and what the company is planning next – he is keeping top secret.” Despite criticism from MPs and NGOs who are calling for more transparency in EU billion-dollar deals, the EU Commission does not want to give any insight into the purchase of vaccines. As with contracts with other manufacturers, the Commission has disclosed a preliminary agreement and a purchase agreement for its business with Pfizer, but essential details such as the delivery price and liability issues have been blacked out in these.
Not only the contracts, even the initiation of the business remains in the dark. The EU Commission rejected a request for freedom of information from netzpolitik.org on the news between Commission chief Von der Leyen and Pfizer boss Bourla in July: “No documents could be found that fall within the scope of your request,” says the Answer by the Secretary-General of the Commission, Ilze Juhansone. In this case, netzpolitik.org lodged a complaint with the ombudswoman O’Reilly. As a result, there was recently a virtual meeting between seven top officials: from the Commission and five from the Ombudsman. In it, the Commission set out in detail how it deals with SMS or messenger services such as WhatsApp and Signal. Such messages are “by their nature short-lived” and are therefore neither used in formal decision-making nor do they produce binding commitments by the institution. As a result, SMS or messenger messages have never been filed in the Commission’s archive system.
Defense Department officials are reviewing whether to make a coronavirus booster shot mandatory for all active-duty and reserve troops, but have not come to any final decisions on the need yet, Pentagon spokesman John Kirby said on Friday. “There are discussions in the department about the efficacy of a booster mandatory policy as well,” he told reporters during a press conference. “Should there be an addition to the [department’s] mandatory vaccine requirement, we will clearly communicate that and be transparent about it.” The Centers for Disease Control and Prevention recommend that all Americans age 16 and older get both the initial two-dose COVID-19 vaccine (or the one-dose version produced by Johnson & Johnson) and a booster shot six months after completing the initial regimen.
Earlier this month, White House officials announced that all eligible Americans should get a booster shot “as soon as possible” to help counter the recent surge in COVID-19 variant cases spreading worldwide. The military services have required all active-duty troops to be vaccinated with the initial doses, and Guard and Reserve troops to get their shots by next summer. Kirby said that more than 96 percent of the active duty force has gotten at least one dose of the vaccine, with 90 percent fully vaccinated. Guard and reserve numbers are significantly lower — for the military as a whole, the fully vaccinated rate is 74 percent. However, some of those numbers could be lower because of a lag in collecting and reporting information from guard and reserve units.
“..more and more forces and equipment are being accumulated on the line of contact in the Donbass, supported by an increasing number of Western instructors.”
The Pentagon has disclosed details of the shipment of anti-tank missile systems and projectiles supplied to Kiev, as Moscow grows increasingly concerned about the prospect of a full-blown conflict in Ukraine’s Donbass region. In a statement received by Russian news outlet TASS on Thursday, Pentagon spokesman Lieutenant Colonel Anton Semelroth said that “the $60 million package… included 30 Javelin command and control launchers, as well as 180 missiles.” According to him, the rocket launchers were delivered to Ukraine on October 23. “In 2021, the US allocated more than $450 million in aid to Ukraine for security tasks as part of our continued commitment to support the country’s ability to defend its sovereignty and territorial integrity,” the spokesman added.
Semelroth’s comments come amid warnings from Moscow over tensions in the war-torn region close to Russia’s borders. Last week, Russian Foreign Minister Sergey Lavrov said that “more and more forces and equipment are being accumulated on the line of contact in the Donbass, supported by an increasing number of Western instructors.” At the end of November, the top diplomat said that claims Ukraine’s troops had deployed American-made Javelin rocket launchers were a matter of grave concern and could lead to a full-blown offensive in the war-torn region. “In recent weeks, we have seen a stream of consciousness from the Ukrainian leadership – especially when it comes to the military – that is excessively inflamed and dangerous,” Lavrov said.
Just hours before, the head of Ukraine’s military intelligence service, Kirill Budanov, revealed that advanced US-made Javelin systems had been tested by Ukraine’s troops and were being used by soldiers in the Donbass. Russia’s ambassador in Washington, Anatoly Antonov, warned the White House earlier in November that supplying Ukraine with deadly armaments could diminish hopes for peace in the region, stating that Moscow believes “another opportunity to encourage Kiev to stop the war has been missed.”
“The op-ed concludes by advising Sullivan to weigh his words carefully going forward and not to “have a big mouth,” lest he “create more embarrassment” for the US.”
A Chinese state-run media outlet has warned Washington that Beijing will not hesitate to strike US forces should they try to prevent China’s reunification with Taiwan, as promised recently by a top American official. The Global Times picked up on National Security Advisor Jake Sullivan’s statement on Tuesday, in which he said that the US was “going to take every action that we can take, from the point of view of both deterrence and diplomacy” to prevent a scenario where China takes over Taiwan militarily. The message was echoed the same day by Secretary of State Antony Blinken, who warned China that a military scenario vis-a-vis Taiwan would be a “very serious mistake.”
However, the Chinese outlet surmised that Sullivan’s assurances should not be construed as a “manifesto of US policy,” as the “US simply cannot build a deterrent to prevent the Chinese mainland from carrying out reunification by force when necessary.” The op-ed goes on to claim that Washington does not really have the “will to defend Taiwan at all costs.” The article takes a yet more bellicose turn when it says it is “credible” that US troops, should they come to Taiwan’s rescue, would be “heavily attacked” by the People’s Liberation Army if “reunification by force” does happen. The Global Times predicts Sullivan would be likely to “recall or downplay” his statement later, since the “US cannot afford” to defend Taiwan “at the cost of a deadly war.”
The op-ed warns that “reunification by force will definitely happen” unless Washington convinces Taiwan authorities to accept the concept of ‘one country, two systems’ and engage with mainland China “on the path of peaceful reunification.” The article blames Taiwan’s ruling Democratic Progressive Party, which came to power in 2016, for the escalation, adding that the situation has possibly already gone beyond the point of no return. The op-ed concludes by advising Sullivan to weigh his words carefully going forward and not to “have a big mouth,” lest he “create more embarrassment” for the US.
This happened on October 27. The High Court, when reading its verdict this week, undoubtedly knew about it.
Jeffrey Sterling @S_UnwantedSpy: “I can guarantee that in a US prison he would not receive medical attention. It took the attention of a US senator for me to receive proper medical attention. #Assange won’t have that “assurance”.
Julian Assange has had a stroke in Belmarsh Prison, his fiancee Stella Moris revealed last night. The WikiLeaks publisher, 50, who is being held on remand in the maximum-security jail while fighting extradition to America, was left with a drooping right eyelid, memory problems and signs of neurological damage. He believes the mini-stroke was triggered by the stress of the ongoing US court action against him, and an overall decline in his health as he faces his third Christmas behind bars. It happened at the time of a High Court appearance via video link from Belmarsh in October. A ‘transient ischaemic attack’ – the interruption of the blood supply to the brain – can be a warning sign of a full stroke. Assange has since had an MRI scan and is now taking anti-stroke medication.
Ms Moris, 38, a lawyer, said: ‘Julian is struggling and I fear this mini-stroke could be the precursor to a more major attack. It compounds our fears about his ability to survive the longer this long legal battle goes on. ‘It urgently needs to be resolved. Look at animals trapped in cages in a zoo. It cuts their life short. That’s what’s happening to Julian. The never-ending court cases are extremely stressful mentally.’ She said he was kept in his cell for long periods and was ‘short of fresh air and sunlight, an adequate diet and the stimulus he needs’. Assange faced a major legal setback on Friday when the High Court overturned a judgment made this year preventing extradition to the US to face charges under the US Espionage Act.
His lawyers successfully argued he would be kept in conditions in the US that could lead to a serious risk of suicide. The High Court reversed the earlier ruling after the US government offered assurances about his potential imprisonment. But Ms Moris said: ‘I believe this constant chess game, battle after battle, the extreme stress, is what caused Julian’s stroke on October 27. He was feeling really unwell, far too ill to follow the hearing, and he was excused by the judge but could not leave the prison video room. ‘It must have been horrendous hearing a High Court appeal in which you can’t participate, which is discussing your mental health and your risk of suicide and in which the US is arguing you are making it all up. ‘He had to sit through all this when he should have been excused. He was in a truly terrible state. His eyes were out of synch, his right eyelid would not close, his memory was blurry.’