

Roy Lichtenstein Woman in Bath 1963

Science can flourish only in an atmosphere of free speech
– Albert Einstein
Pfizer Purchase Agreement
McCullough: 3-5 years of turmoil
Peter A. McCullough, MD, MPH: Something is gone very wrong in the world; I think we are in for about 3-5 year period of turmoil… pic.twitter.com/NAkpNksmRF
— Camus (@camus37) July 25, 2021
Fleming: what’s in the vaccines?
Shocking if true… pic.twitter.com/kithILe24l
— Camus (@camus37) June 30, 2021
Weinstein Tucker
Bret Weinstein – worrisome if true… pic.twitter.com/4tbF6MSceX
— Camus (@camus37) July 26, 2021
Bret Weinstein about vaccines…. pic.twitter.com/xdADwwb1Rr
— Camus (@camus37) July 27, 2021
Twitter thread.
Since the “vaccines” have only been used for some 5 months, this means: “To infinity and beyond!”.
And since Covid is so similar to the flu, what happens if you catch that next year, or the one after that?
• Spike Protein Is Still Circulating 5 Months From Vaccination (VT)
Robert Malone has said you need to measure duration, distribution, and amount for the spike protein. FDA never did this; one of our researchers did. They found spike protein is still circulating 5 months from vaccination in 100% of patients tested (6 people; random pick). And yes, they plan to publish this. But I wanted to give our followers advance notice. One of the 6 had spike in 15% of his monocytes!!! This is NOT limited to 5 months out… This could last for years, we just don’t know yet. The 6 were randomly picked. They wanted to use them as “healthy controls.” Then the researchers freaked out when they found this. Whoa. Anyone can verify this but nobody in academia will attempt to do this. The results will be too embarrassing. It will prove Malone was right the whole time about importance of measuring those 3 things. He said this on the Darkhorse podcast that was censored on YouTube.
THIS IS NOT NORMAL. The antigen is supposed to stick around for a week or two and vanish. Is it any wonder why people who have been vaccinated have long term symptoms? Part of this is permanent damage caused by the inflammation (which causes scarring which doesn’t heal)… The antigen (in this case spike) is SUPPOSED to disappear in 2 weeks. So this can explain long-term vaccine symptoms (along with permanent or temp damage from the inflammation and blood clots caused by the vaccine). Permanent damage is from scarring caused by inflammation. Anyone can replicate this if they have the proper assays. Will anyone? Will they be able to get it published? That’s the big question. Journals censor by deeming unfavorable research as “out of scope” for the journal.
The spike proteins stay, but they don’t protect you (any longer, if they ever did).
• Early Vaccinees Are Twice As Likely To Catch Covid As Later Recipients (ToI)
People vaccinated before late February are twice as likely to catch the coronavirus than other inoculated Israelis, according to new research. “We looked at tens of thousands of people tested in the month of June, alongside data on how long had passed since their second shot, and found that those vaccinated early were more likely to test positive,” Dr. Yotam Shenhar, who headed the research, told The Times of Israel. “This definitely reinforces the argument for giving a third vaccine dose to the elderly.” The report, published by the healthcare provider Leumit, comes on the heels of other Israeli studies that suggest a decreasing vaccine effectiveness, partly as a result of the Delta variant and partly because of the passage of time. However, British data indicates the Israeli studies may be overstating the case.
Data released by the Health Ministry on Thursday suggested that people vaccinated in January were said to have just 16% protection against infection now, while in those vaccinated in April the effectiveness was at 75%. The Leumit study looked only at the apparent waning of protection over time, and divided the vaccinated population into two based on inoculation dates, comparing early vaccinators to late vaccinators. Shenhar, head of Leumit’s labs, acknowledged that the early vaccinators group includes many people who raced to get shots because they have underlying illnesses, which may make them more vulnerable to infection. But he said that could not fully account for the stark effect seen in the data. Shenhar said the data should prompt the government to seriously consider booster shots for over-70s.
[..] In his study, the apparent waning effect in immunity was felt across all ages. For all age groups, early vaccinators were 1.95 times more likely to be confirmed coronavirus positive. Among those aged 60-plus, early vaccinators are twice as likely to get infected. For those aged 40-59 early vaccinators are 2.1 times more vulnerable, and among under 39s they are 1.6 more likely to catch the coronavirus. “In a previous analysis we showed that as time passes since the vaccine, the level of antibodies drops at a rate of about 40% per month. This new study builds a clearer picture of the effect seen in the months after vaccination,” said Shenhar.
As I said in Rage Against the Vaccine, we are finding out that the vaccinated are the spreaders. This is such a blow to the official story, they’ll deny it as long as possible.
• New Mandate That MUST Be Enforced NOW (Denninger)
Work in health care? I don’t care if you are in direct patient-care or not; if you work in a medical facility of any sort this applies to you if you took the jab. We now know if you become infected with Covid, and you had the jab, you will have a higher viral titer before becoming symptomatic, if you become symptomatic at all. That is, you, compared against someone who did not take the jab where you are both infected, are much more likely to transmit the virus to someone else before knowing if you get infected. Since viral replication occurs in hours per cycle, not days, testing, unless on an every day basis, is not sufficient to detect the risk. Nearly everyone coming into a medical facility is at heightened risk of one sort or another; people do not, generally-speaking, go into medical facilities if all is well. This is certainly true for hospitals and “urgent care” facilities.
Masks cannot mitigate this risk as the virus is in aerosols and when you exhale you will thus project it into the environment if it is present. It does not matter if you use an N95 or surgical mask; an N95 will still break the seal around your face when you exhale to some extent and thus you will exhale virus if you are infected. Therefore if you work in such a facility and you took the jab, given what we now know, you are hereby obligated from now until forever into the future, until Covid and any future mutation of it is no longer of material concern, obligated to use both Ivermectin on an every 3-day basis, and Budesonide on an every day basis, both as prophylaxis. This obligation is now attached and permanent so long as you remain employed.
Since people believe that there is nothing wrong with mandating people take non-sterilizing shots to work in health care then, given that you ****ed up and are now putting people at grossly-enhanced risk there is also nothing wrong with this mandate either. Said prophylaxis is to take place on video and be recorded each day for the Budesonide and every three days for Ivermectin. If you refuse you are fired and your medical credentials are stripped. If you infect someone without documented proof that you have taken this prophylaxis as a medical worker and have been jabbed you are charged with felony assault and if they die you are charged with depraved indifference homicide, which in most jurisdictions is Murder 2. If law enforcement will not bring these charges then the relatives of said person who is impacted has every moral and ethical right to personally enforce the appropriate penalties.
A comment at Naked Capitalism confirms it once more: it’s the vaccinated. Who are free to travel, eat indoors etc., … and free to spread the virus.
• About The French Guyana Paper From The CDC (IM Doc)
This is how science – the actual process – not the Fauci version – should be working. I have repeatedly stated that I am seeing much much more vaccinated positives than one would ever have expected. As I have stated, they seem to be much sicker (though not critically so) and they tend to happen in clusters. For the past two months, this has stuck out from the dominant media narrative. I have never had to fight the cognitive dissonance between the media and my own eyeballs in my life. I belong to a large non-public alumni group of my residency program that has literally thousands of IM docs all over America. The first thing a scientist does is to confirm that your observations are general or something you are just seeing. It was quickly obvious from that group that I was far from alone despite the “minimal breakthrough cases” media narrative.
So, then you do everything you can to hypothesize reasons why you are seeing what you are. I have been a physician for 30 years and that experience plays a huge role as well. Having this gigantic number of breakthrough cases just simply does not happen. I continue to see more than half the cases in vaccinated patients and so do many others. UNHEARD OF IN VACCINES BEFORE NOW. Part of hypothesizing why is looking to the literature for evidence. Seldom is this found in RCT at this stage. Case reports and series like this paper are critical. They are seeing the same breakthrough ratio. And they have done a lot more viral research than you can. This is a gold mine for my own questions.
Is there anything in the paper that could possibly explain what I am seeing. Lots of times, it is not in the headline part but in all the test results and discussion. And yes, there is a very important finding deep in the results. Why would clustering and sicker patients be so much more common in the breakthrough patients. – there must be a reason for that? If you look at the brief discussion of cT or cycle threshold you will see that the vaccinated patients have a SIGNIFICANTLY lower cT than the unvaccinated. That is the way the PCR test works. It basically means the vaccinated have a much higher amount of viral active particles than the unvaccinated. That would account for the breakthroughs I and my colleagues are seeing being a bit more ill. And it would explain the clustering.
The vaccinated breakthroughs have much higher viral load so they are much more contagious and the higher viral load makes them more symptomatic. So we now have a suggestion and strong evidence that the vaccinated population may be spreading much more virus than the unvaccinated. I would say that is a critical public health issue and must be further researched immediately. This Certainly needs much more work. THis is not confirmatory of any conclusions. But it is consistent with observation on the ground – unlike most of what the media has been spewing to the American people. But this is how science works. This paper is about the gamma variant but a conference yesterday with experts discussed that similar findings were being found in delta and lambda.
The suggestion in this paper is now on the front of my mind. I am even now thinking of ways to confirm or falsify these conclusions going forward. This is science. Another issue. The writers make the point that the breakthrough rate is extremely divergent from the expected rate. The difference is this paper documents what is happening in REAL LIFE. So much of what we are hearing on our media about vaccine efficacy is research being done in vitro. It is presented as gospel truth. I just want to scream.
Maybe the next big wave after Delta will make people listen to VanDen Bossche.
• A Last Word of Caution (VanDen Bossche)
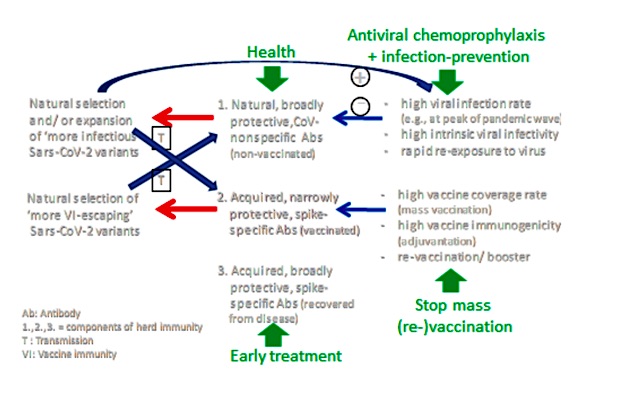
The current expansion in prevalence of infectious Sars-CoV-2 variants is highly problematic because it erodes natural Ab-based, variant-nonspecific immunity in the non-vaccinated part of the population. The high infectivity rate that results from this expansion not only further enhances the expansion of these variants but may also drive natural selection of viral variants that are featured by an even higher level of infectiousness. Erosion, therefore, of natural Ab-based, variant-nonspecific immunity promotes breeding and transmission of more infectious viral variants in the non-vaccinated part of the population. On the other hand, mass vaccination promotes natural selection of increasingly vaccine immunity (VI)-escaping variants in the vaccinated part of the population.
Taken together, mass vaccination conducted on a background of high infectivity rates enables more infectious, increasingly VI-escaping variants to expand in prevalence. This evolution inevitably results in inclining morbidity rates in both, the non-vaccinated and vaccinated population and precipitates the emergence of circulating viral variants that will eventually fully resist vaccine-mediated immunity (VMI). This is why mass vaccination campaigns should not be conducted during a pandemic of a highly mutable virus, let alone during a pandemic of more infectious variants (unless transmission-blocking vaccines are used!). It is critical to understand that a rapid decline in viral infectivity rates that is not achieved by natural infection but merely results from expedited mass vaccination campaigns will only delay abrupt propagation of emerging, fully vaccine-resistant viral variants and hence, only delay the occurrence of a high wave of morbidity and mortality.
In contrast, mass vaccination campaigns that are progressing more slowly, especially when conducted on a background of relatively low infectious pressure, will result in a steadily growing propagation of increasingly VI-escaping variants and hence, cause a wave of morbidity and mortality that continues to grow bigger and larger as more and more people become vaccinated. It’s only when fully vaccine-resistant viral variants will become dominant that this wave will start to peak. To prevent more detrimental consequences of the ongoing evolution of Sars-CoV-2, we have no choice but to mitigate erosion of natural, Coronavirus (CoV)-nonspecific immunity in non-vaccinated individuals and exertion of strong immune selection pressure on immunodominant vaccinal epitopes in vaccinated individuals.
This is to say that we must stop mass vaccination and lower viral infectivity rates immediately. Continued mass vaccination will only lead to a further increase in morbidity and hospitalization rates, which will subsequently culminate in a huge case fatality wave when expansion of more infectious, vaccine-resistant variants will explode.
No kidding.
• Journalists: Covid-19 News ‘Censored’ To Create ‘One Official Narrative’ (PG)
Elijah, who came up with the group’s name and found it “therapeutic” to talk to others with the same concerns, told Press Gazette: “It’s been unprecedented the way Covid-19 has been reported in the UK but not just in the UK, worldwide. “There’s only been one official narrative played out in the mainstream media and that has not changed over time. “There’s only been one ‘scientific truth’ allowed to be discussed: the one endorsed by worldwide governmental regulatory bodies, even that has been very selective. This has given the public a distorted view of the truth which has been highly damaging.” Elijah said her biggest concern was about “censorship” of information online that goes against this narrative and referred to the Trusted News Initiative, through which the BBC, other publishers and tech giants flag up the most dangerous disinformation to each other.
“For a long time, we’ve been in this dark era of censorship that’s been embodied by the Trusted News Initiative which cuts across big tech and all mainstream media,” she said. “It’s been packaged around this war on disinformation or misinformation- where anything that’s gone against the official narrative has not just been ‘fact checked’ but has been suppressed or removed.” Ex-BBC radio journalist Gosling told Press Gazette he had interviewed two doctors who shared counter-narratives – Dr Tess Lawrie of the Evidence-based Medicine Consultancy in Bath who called for early treatment to take place post-Covid diagnosis, and Florida-based immunologist Dr Stanley Laham who called for the use of ivermectin and warned against the use of the approved but “experimental” vaccines – but that both were removed from Youtube on grounds of misinformation.
Gosling said he wanted to speak out against fear-inducing and sometimes inaccurate coverage. He pointed as one example to a BBC Newsround segment last month in which a contributor claimed the Pfizer vaccine was “100% safe” for 12 to 15-year-olds. Gosling submitted a complaint about the “shocking” and “disgusting” claim and the BBC has since removed the claim from the online article and video and published a correction. Gosling said: “Our main concern is that there’s a very powerful lobby behind many of these Covid measures, including treatment, lack of treatment and vaccines, obviously, but there isn’t much of a lobby in the other direction. And I think most of us feel that our employers of various sorts have not been representing both sides.”
“Deaths began to fall in February. After March 1 – when only 1 in 13 Americans were fully vaccinated – they plunged further. In the five months since, perhaps 80,000 people have died from (or with) Covid – fewer than died in January alone.”
But as I said, even putting aside the issue of how we classify the partially vaccinated, Fauci and Murthy lied about what percentage of coronavirus deaths are now occurring in FULLY vaccinated people. It is much higher than the sub-1 percent figures they offered. This fact should have been obvious to anyone who has seen the data from England, Scotland, and Israel. Those countries vaccinated a greater percentage of their populations more quickly than the United States. They have also been much more transparent about reporting hospitalizations and deaths among vaccinated people. And in all three countries, hospitalizations and deaths have spiked since May – and vaccinated people have accounted for more than HALF of all deaths recently.
The difference does not come from the type of vaccines, either. Israel used only the Pfizer vaccine, which until recently was considered the better of the two mRNA vaccines. The United Kingdom gave many Pfizer doses too. So the comments from Fauci and Murthy defied credibility – how could other countries have so many more deaths in their vaccinated populations? The answer is that Fauci and Murthy are – intentionally – using the wrong denominator. They say “now” or “are.” But they are comparing deaths among the fully vaccinated – which have essentially been an issue only since May – with ALL deaths beginning from the day the United States offered its FIRST vaccine dose (or even possibly from the beginning of the epidemic).
The United States has had roughly a quarter-million deaths from Covid this year (the CDC reports 216,000, a number that will rise somewhat). It has had closer to 300,000 since the first dose was offered on Dec. 14. But more than half those deaths occurred in December and January, when essentially no one was fully vaccinated. Not even 2 percent of Americans were fully vaccinated as of February 1. Deaths began to fall in February. After March 1 – when only 1 in 13 Americans were fully vaccinated – they plunged further. In the five months since, perhaps 80,000 people have died from (or with) Covid – fewer than died in January alone.
Vaccine advocates rarely acknowledge the fact that deaths started dropping long before most people had received shots. In reality, even acknowledging that many people who received vaccines in January and February were older and vulnerable, seasonality and herd immunity seem to have had a greater impact on broad Covid trends than vaccinations.
But are noted as Covid admissions.
• Most Covid Patients In UK Hospitals Only Tested Positive After Admission (ZH)
Over half of those hospitalized with Covid-19 in the UK only tested positive after admission – suggesting that “vast numbers are being classed as hospitalised by Covid when they were admitted with other ailments, with the virus picked up by routine testing,” according to The Telegraph, citing leaked government figures. The takeaway? Oft-cited statistics published daily may far overstate Covid hospitalizations – and consequently, pressures on the National Health Service (NHS).
“The leaked data – covering all NHS trusts in England – show that, as of last Thursday, just 44 per cent of patients classed as being hospitalised with Covid had tested positive by the time they were admitted. The majority of cases were not detected until patients underwent standard Covid tests, carried out on everyone admitted to hospital for any reason. Overall, 56 per cent of Covid hospitalisations fell into this category, the data, seen by The Telegraph, show. Crucially, this group does not distinguish between those admitted because of severe illness, later found to be caused by the virus, and those in hospital for different reasons who might otherwise never have known that they had picked it up.” -Telegraph
In June, UK health officials instructed NHS trusts to provide “a breakdown of the current stock of Covid patients” between those who were hospitalized primarily for Covid and those admitted for other reasons. Thus far, the NHS has failed to publish this now-leaked information. Breaking it down, out of more than 780 hospitalizations dated last Thursday, 44% tested positive within 14 days prior to admission, while 43% tested positive within two days of admission, and 13% tested positive ‘in the days and weeks that followed’ – including those likely to have caught the virus in the hospital. “Experts said the high number of cases being detected belatedly – at a time when PCR tests were widely available – suggested many such patients had been admitted for other reasons,” according to the report.
Plasma.
• A Long-term Perspective On Immunity To COVID (Nature)
Immunological memory is not a long-lasting version of the immediate immune reaction to a particular virus; rather, it is a distinct aspect of the immune system. In the memory phase of an immune response, B and T cells that are specific for a virus are maintained in a state of dormancy, but are poised to spring into action if they encounter the virus again or a vaccine that represents it. These memory B and T cells arise from cells activated in the initial immune reaction. The cells undergo changes to their chromosomal DNA, termed epigenetic modifications, that enable them to react rapidly to subsequent signs of infection and drive responses geared to eliminating the disease-causing agent4. B cells have a dual role in immunity: they produce antibodies that can recognize viral proteins, and they can present parts of these proteins to specific T cells or develop into plasma cells that secrete antibodies in large quantities.
About 25 years ago5, it became evident that plasma cells can become memory cells themselves, and can secrete antibodies for long-lasting protection. Memory plasma cells can be maintained for decades, if not a lifetime, in the bone marrow6. The presence in the bone marrow of long-lived, antibody-secreting memory plasma cells is probably the best available predictor of long-lasting immunity. For SARS-CoV-2, most studies so far have analysed the acute phase of the immune response, which spans a few months after infection, and have monitored T cells, B cells and secreted antibodies7. It has remained unclear whether the response generates long-lived memory plasma cells that secrete antibodies against SARS-CoV-2.
Turner and colleagues took up the challenge of identifying antibody-secreting memory plasma cells in the bone marrow of people who have recovered from COVID-19 (called convalescent individuals). Memory plasma cells are rare, and those specific for a particular disease-causing agent will obviously be extremely scarce. Nevertheless, Turner and colleagues detected memory plasma cells that secreted antibodies specific for the spike protein encoded by SARS-CoV-2 in 15 of 19 individuals, approximately 7 months after infection. Notably, when the authors obtained samples 4 months later (11 months after SARS-CoV-2 infection), the number of such plasma cells had remained stable in all but one of the individuals analysed. Those plasma cells did not proliferate, which classifies them as bona fide memory plasma cells. Their numbers equalled those of memory plasma cells found in the individuals after vaccination against tetanus or diphtheria, and which provide long-term immunity to those diseases.
When Turner et al. tracked the concentrations of antibodies against SARS-CoV-2 in the individuals’ blood serum for up to one year, they observed a biphasic pattern (Fig. 1). In the acute immune response around the time of initial infection, antibody concentrations were high. They subsequently declined, as expected, because most of the plasma cells of an acute immune response are short-lived. After a few months, the antibody concentrations levelled off and remained more or less constant at roughly 10–20% of the maximum concentration observed. This is consistent with the expectation that 10–20% of the plasma cells in an acute immune reaction become memory plasma cells5, and is a clear indication of a shift from antibody production by short-lived plasma cells to antibody production by memory plasma cells. This is not unexpected, given that immune memory to many viruses and vaccines is stable over decades, if not for a lifetime8.
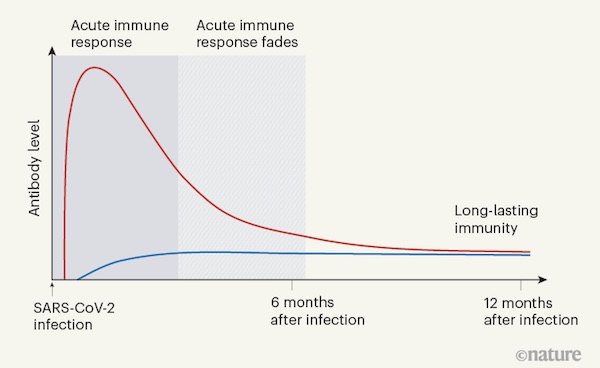 Figure 1 | The immune response to SARS-CoV-2 infection. Data are becoming available that shed light on longer-term aspects of the human immune response to coronavirus infection. One component of the defence response is the production of antibodies that target viral proteins (red line). During the initial, acute phase of the immune response, antibody levels peak rapidly; this peak is generated by short-lived immune cells called plasma cells. Turner et al.1 present clinical evidence, from people who have had COVID-19, that long-lived, memory plasma cells that produce antibodies are generated in the bone marrow. These cells provide long-term antibody production that offers stable protection at a level of 10–20% of that during the acute phase (blue line). Memory plasma cells are a cell type that can be maintained for many years, if not a lifetime. Wang et al.2 have characterized antibody responses at between six months and a year in people who have been infected with SARS-CoV-2; their results also provide evidence for the generation of immunological memory.
Figure 1 | The immune response to SARS-CoV-2 infection. Data are becoming available that shed light on longer-term aspects of the human immune response to coronavirus infection. One component of the defence response is the production of antibodies that target viral proteins (red line). During the initial, acute phase of the immune response, antibody levels peak rapidly; this peak is generated by short-lived immune cells called plasma cells. Turner et al.1 present clinical evidence, from people who have had COVID-19, that long-lived, memory plasma cells that produce antibodies are generated in the bone marrow. These cells provide long-term antibody production that offers stable protection at a level of 10–20% of that during the acute phase (blue line). Memory plasma cells are a cell type that can be maintained for many years, if not a lifetime. Wang et al.2 have characterized antibody responses at between six months and a year in people who have been infected with SARS-CoV-2; their results also provide evidence for the generation of immunological memory. Where finance and Covid meet. These guys are good at spotting trends.
• Decline In UK COVID Cases Signals Coming “Inflection” For US (ZH)
Just one week ago, as Dr. Anthony Fauci was cranking the Delta variant “fearmongering” up to 11 once again, JPM’s Croatian quant Marko Kolanovic was telling the bank’s clients that a looming inflection point for new cases in the UK (widely seen as a leading indicator for the direction of new cases in the US) would soon arrive, kick-starting demand for value stocks and reopening plays. Although Kolanovic is a Wall Street quant, not an epidemiologist, it turns out his view was correct. Because one week later, the number of new cases being confirmed in the UK and EU has fallen, even as the UK’s “Freedom Day” has come and gone. Deutsche Bank’s Jim Reid described the decline in new cases in the UK “nothing short of remarkable”.
According to Reuters data, the number of new cases fell for a sixth consecutive day, to 24,950 on Monday from 29,173 on Sunday. The total number of new cases over the past week, at just over a quarter of a million, is more than 20% lower than the prior week. While the UK’s economy-crippling “pingdemic” continues, and many have continued to isolate, meaning the UK is still a way’s away from achieving a return to “normality”. Additionally, despite the fast rise of cases to near peak levels, mortality is currently 95% lower than during the January peak. This should give confidence to investors that delta is not a serious threat to global growth. If the US follows the template of the UK, daily cases might be peaking in the next 12 days…while we think Energy-Epicenter stocks are going to start to rally beginning this week.
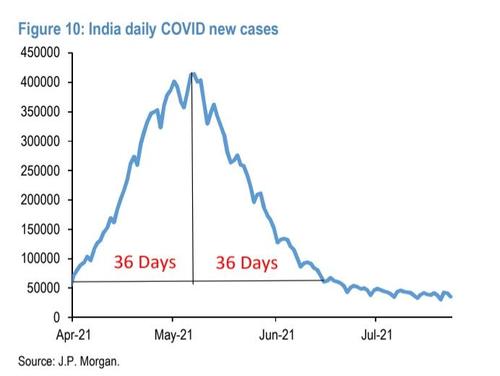
While the Delta variant continues to dominate “our discussions with clients,” Kolanovic claimed that fears about the variant are overblown. The UK, he added, appears to be following a timeline similar to what the world saw in India. This should give confidence to investors that Delta isn’t a serious threat to global growth. Well, that and the drop in mortality. Speaking of markets, Kolanovic suggested that this is the start of a rotation into cyclicals. Some might be tempted to attribute the drop in UK cases to a fluke, or the pingdemic, or some other factor. But as Kolanovic reminds us, the trajectory of India’s recent COVID flareup (the first national outbreak to be caused by the delta variant) was similarly swift, as JPM illustrates with a handy chart.
Censorship is everywhere. Because it offers total control.
• In a Hall of Mirrors You Have To Break Some Glass To See Clearly (Kunstler)
I’ll tell you what’s really funny: the new Sam Harris “Making Sense” podcast with Dr. Eric Topol, veep of Scripps Research. These two just can’t make sense of why the folks outside their Southern California smuggery bubble have any reservations about getting vaxed-up against Covid-19. It’s like a mental illness to them — all these selfish, Trump-driven, flag-smooching ignoramuses beyond the pale of Wokery, who are putting at risk their science-loving betters in the PhD hives of the New Normal, while that King Kong of Covid variants (code-name Delta) rages through the hillsides and canyons beneath Mulholland Drive. The insolence! Can’t these morons just follow simple instructions (available 24/7 at CNN)?
Okay, here’s why, Sam and Eric: Because every institution in American life has squandered its credibility in the service of a political program that seeks to destroy whatever used to be worth caring about in Western Civ, including free thought, free speech, free inquiry, free movement, truth, beauty, and the right to resist official coercion. Half the country has no trust in the government’s public health apparatus, led by the — shall we say — slippery Dr. Anthony Fauci. Should they believe NPR? The New York Times? CBS-News? Should they follow every bob and judder of Rachel Maddow’s Adam’s apple? Should they swallow every globule of obvious horse-shit served up by Jen Psaki?
Hey Sam and Eric, have you followed what went on in the US Department of Justice and the FBI the past five years, these supposed redoubts of rectitude? The manufactured “Russian Collusion” hoax? The official lying to FISA courts? The malicious prosecutions? The transparently seditious activities of CIA agent Eric Ciaramella & Co.? The hiding of Hunter Biden’s evidence-stuffed laptop? The enlistment of Facebook, Twitter, and Google in suppression of the news and censorship of opinion? Do you expect people to believe that the basement-haunting “Joe Biden” won an election with those slim victories in the Wokester-controlled, fraud-drenched city precincts of Philadelphia, Atlanta, Milwaukee, and Detroit? Or that Merrick Garland and Christopher Wray wouldn’t lie about it?
Pelosi helping Putin ridicule America.
• The Jan. 6th Show Trials Threaten All of Us (Ron Paul)
The recent felony conviction and eight month prison sentence of January 6th protester Paul Hodgkins is an affront to any notion of justice. It is a political charge and a political verdict by a political court. Every American regardless of political persuasion should be terrified of a court system so beholden to politics instead of justice. We’ve seen this movie before and it does not end well. Worse than this miscarriage of justice is the despicable attempt by the prosecutor in the case to label Hodgkins – who has no criminal record and was accused of no violent crime – a “terrorist.” As journalist Michael Tracey recently wrote, Special Assistant US Attorney Mona Sedky declared Hodgkins a “terrorist” in the court proceedings not for committing any terrorist act, not for any act of violence, not even for imagining a terrorist act.
Sedky wrote in her sentencing memo, “The Government … recognizes that Hodgkins did not personally engage in or espouse violence or property destruction.” She added, “we concede that Mr. Hodgkins is not under the legal definition a domestic terrorist.” Yet Hodgkins should be considered a terrorist because the actions he took – entering the Senate to take a photo of himself – occurred during an event that the court is “framing…in the context of terrorism.” That goes beyond a slippery slope. He is not a terrorist because he committed a terrorist act, but because somehow the “context” of his actions was, in her words, “imperiling democracy.” In other words, Hodgkins deserved enhanced punishment because he committed a thought crime.
The judge on the case, Randolph D. Moss, admitted as much. In carrying a Trump flag into the Senate, he said, Hodgkins was, “declaring his loyalty to a single individual over the nation.” As Tracey pointed out, while eight months in prison is a ridiculously long sentence for standing on the floor of the “People’s House” and taking a photograph, it is also a ridiculously short sentence for a terrorist. If Hodgkins is really a terrorist, shouldn’t he be sent away for longer than eight months?
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Fauci masks
Video: Fauci talking out of both sides of his mouth. The mask charade is over. What a fiasco! pic.twitter.com/JHJJ5ijReS
— Justin Hart (@justin_hart) July 27, 2021
Support the Automatic Earth in virustime. Click at the top of the sidebars to donate with Paypal and Patreon.
