
Doc Robinson
Forum Replies Created
-
AuthorPosts
-
Doc Robinson
ParticipantFrom above:
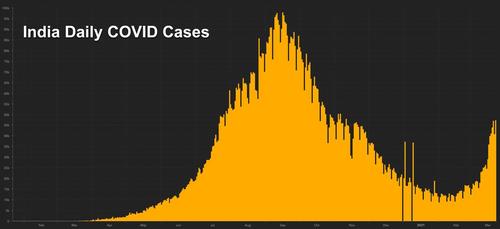
That graph of India’s cases can be misleading, since there is no comparison to other countries to give some perspective. The number of cases per million people is what’s relevant.
The total cases per million in the US, and the total covid deaths per million in the US, are more than 10 times the numbers for India.
India’s curve gets flattened when compared to the US curve in the same chart:
Our World In Data – India vs USParticipantWhen my father was dying, I remained at his bedside for his final days. The last few days he was primarily in a coma from which he would rouse himself from time to time. . . . I would hold his hand and say my prepared speech: “Go to the light,” and “Now is your chance to get out of this body.” I’m pleased that I did that; those are all the right things to say when someone is dying. (“You’ve done a good job in this lifetime.” “Everybody loved you.” “It’s time to move on. . . .”). . . . Very near the end, he began a siege of apnea, and I leaped to my feet, beginning my talk about “Go to the light.” He opened his eyes, and he looked at me and said quite clearly, “You know, it’s not that big of a deal.”
From the book It’s Easier Than You Think, by Sylvia Boorstein
A quote from the Dalai Lama:
My religion is very simple. My religion is kindness.ParticipantThe Hawaii story (of fully vaccinated people still being infected) is happening in other states, too, every other state. They are being called “breakthrough cases.” The vaccines never were 100% effective, so that leaves a certain percentage right off the bat for whom the vaccines will be ineffective. Plus, the ever-mutating and evolving variants of the virus can have a spike that’s different from what the vaccine targets, different enough to evade whatever defenses the body made in response to the vaccine.
ParticipantNext week, there is expected to be some movement with the Julian Assange case. The High Court hasn’t yet decided whether to allow the US to proceed with its appeal of the ruling that denied extradition.
“I want to remind everyone it’s been 2 years since Julian Assange has been [locked away] in a high security prison. He faces 175 years in prison for the same reason he has been nominated for the Nobel Peace Prize.”
—@suigenerisjen“Assange was still locked up even though he had never been convicted of any crime.”
itwire.com/strategy/labor-mp-hill-calls-for-government-to-step-up-and-bring-assange-home.html
Stella Moris #DropTheCharges @StellaMoris1
·Feb 18
New: The Court has now granted Julian’s team an extension until March 29th to reply to the US appeal grounds/cross-appeal. The High Court will decide whether it will allow the US permission to appeal after March 29th.ParticipantHere’s another troubling issue about the Covid vaccine trials for infants and children…
Such clinical trials, if they don’t give the desired results, tend to get dropped and the results aren’t made public. This is problematic for a bunch of reasons.
Children enrolled in these studies are subjected to risks. If the results are kept secret by the drug companies, then the risks aren’t really being imposed for the advancement of science, they are being imposed on children to merely determine whether a certain treatment could be profitable for the drug companies.
The withholding of negative results is also problematic because this “tends to distort the entire medical literature to make a given intervention [like vaccination] look more effective than it really is.”
Nearly a Third of Medical Studies Involving Children Are Never PublishedThe study authors combed through two years’ worth of pediatric trials registered on clinicialtrials.gov, a national registry run by the U.S. government. They found that 19 percent of these trials ended early, and 30 percent of completed trials were never published. That means that [during two years] more than 77,000 children were enrolled in trials that went nowhere..
Testing new drugs in children is fraught with issues of consent, safety, and profit…
Sometimes scientists are reluctant to publish data for trials where results were neutral or negative. Science has a history of favoring studies that show what does work and ignoring studies that show what doesn’t work. But both results are equally important, says Jones.
“Because ‘negative’ trials are generally less likely to be published than ‘positive’ trials, nonpublication tends to distort the entire medical literature to make a given intervention look more effective than it really is,” he said.
http://www.healthline.com/health-news/many-medical-studies-involving-children-never-finished
ParticipantGerm: “Did you know that last year Yale investigated how to guilt-trip people into taking the COVID vaccine?”
That’s worth a closer look, for some indication of what arguments and social pressure to expect. Interesting that this study started in early July 20, and it presents preconceived “facts” about Covid vaccines which didn’t really exist then.
Baseline message… about the effectiveness and safety of vaccines.
Personal freedom message… about how COVID-19 is limiting people’s personal freedom and by working together to get enough people vaccinated society can preserve its personal freedom.
Economic freedom message… about how COVID-19 is limiting peoples’s economic freedom and by working together to get enough people vaccinated society can preserve its economic freedom.
Self-interest message… that COVID-19 presents a real danger to one’s health, even if one is young and healthy. Getting vaccinated against COVID-19 is the best way to prevent oneself from getting sick.
Community interest message… about the dangers of COVID-19 to the health of loved ones. The more people who get vaccinated against COVID-19, the lower the risk that one’s loved ones will get sick. Society must work together and all get vaccinated.
Economic benefit message… about how COVID-19 is wreaking havoc on the economy and the only way to strengthen the economy is to work together to get enough people vaccinated.
Guilt message… about the danger that COVID-19 presents to the health of one’s family and community. The best way to protect them is by getting vaccinated and society must work together to get enough people vaccinated. Then it asks the participant to imagine the guilt they will feel if they don’t get vaccinated and spread the disease.
Embarrassment message… about the danger that COVID-19 presents to the health of one’s family and community. The best way to protect them is by getting vaccinated and by working together to make sure that enough people get vaccinated. Then it asks the participant to imagine the embarrassment they will feel if they don’t get vaccinated and spread the disease.
Anger message… about the danger that COVID-19 presents to the health of one’s family and community. The best way to protect them is by getting vaccinated and by working together to make sure that enough people get vaccinated. Then it asks the participant to imagine the anger they will feel if they don’t get vaccinated and spread the disease.
Trust in science message… about how getting vaccinated against COVID-19 is the most effective way of protecting one’s community. Vaccination is backed by science. If one doesn’t get vaccinated that means that one doesn’t understand how infections are spread or who ignores science.
Not bravery message… describes how firefighters, doctors, and front line medical workers are brave. Those who choose not to get vaccinated against COVID-19 are not brave.
Primary Outcome Measures :
Intention to get COVID-19 vaccineSecondary Outcome Measures :
Vaccine confidence scale… to assess the impact of the messages on vaccine confidence.
Persuade others item… This is a measure of a willingness to persuade others to take the COVID-19 vaccine.
Fear of those who have not been vaccinated… This is a measure of a comfort with an unvaccinated individual visiting an elderly friend after a vaccine becomes available
Social judgment of those who do not vaccinate… This is a scale composed of 4 items measuring the trustworthiness, selfishness, likeableness, and competence of those who choose not to get vaccinated after a vaccine becomes available
ParticipantCorrection:
Despite the “extensive” trials and assurances of safety by the FDA, the fully approved [Rotashield] vaccine actually caused unexpected damage to children, and the vaccine license was finally revoked in the US after nine months of dosing infants with it.(This vaccine was administered orally)
f
ParticipantThe title of that article in Nature is “Ethics of vaccine research.” It gives some guidelines about using children for vaccine testing.
“The amount of research risk to which children can be exposed without corresponding benefit is limited by regulation in US-sponsored research. Because children cannot protect their own interests through informed consent, parents and guardians are asked for permission to enroll their children in vaccine research. Investigators and institutional review boards (IRBs) should ensure that parents and guardians are well informed and make decisions compatible with the interests of the child.”
“An ethical requirement of all clinical research is to minimize risk and maximize benefit.”
“Once a proposal is deemed valuable, valid and acceptable with respect to risks, benefits and subject selection, individuals are recruited and asked for informed consent. Although widely valued, informed consent is imperfectly realized in clinical research. Because massive public education campaigns promote the use of vaccines for public health, individuals may not appreciate how experimental vaccines differ in the context of research… Although little is known about the degree to which participants understand that some of them or their children will (must) get the disease or infection to prove efficacy, this knowledge is likely to be low.”
“When an entire community is randomized to receive an investigational vaccine, strategies for upholding the right of individuals to refuse participation or to withdraw from the research while ‘saving face’ should be sought.”
Ethics of vaccine research
by Christine Grady, Nature Immunology, May 2004
https://www.nature.com/articles/ni0504-465ParticipantRegarding Covid vaccine testing and use in infants and children…
A 2004 article in the journal Nature calls vaccines “one of the miracles of modern science” and praises their “brilliant successes,” but it also mentions a lesser-known failure:
“An effective rotavirus vaccine was pulled from the US market because of a high incidence of intussusception in vaccinated children. Consequently, debates ensued about proceeding with large trials planned in developing countries…”
What is intussusception?
“Intussusception (in-tuh-suh-SEP-shun) is a serious condition in which part of the intestine slides into an adjacent part of the intestine. This telescoping action often blocks food or fluid from passing through. Intussusception also cuts off the blood supply to the part of the intestine that’s affected.” (Mayo Clinic)Did this vaccine actually cause the intussusception in children, after it successfully went through the FDA’s process for full approval and licensing (not just an EUA)? The answer is yes, straight from the CDC’s mouth:
Q: Did RotaShield® vaccine cause intussusception?
A: In the United States, some infants developed intussusception (defined below) soon after RotaShield® was licensed in August 1998… The results of the investigations showed that RotaShield® vaccine caused intussusception in some healthy infants younger than 12 months of age who normally would be at low risk for this condition. The risk of intussusception increased 20 to 30 times over the expected risk for children of this age group within 2 weeks following the first dose of RotaShield® vaccine.http://www.cdc.gov/vaccines/vpd-vac/rotavirus/vac-rotashield-historical.htm
Despite the “extensive” trials and assurances of safety by the FDA, the fully approved vaccine actually caused unexpected damage to children, and the vaccine license was finally revoked in the US after nine months of injecting infants with it.
(comment continued below)
ParticipantParticipant• Fauci Claims Babies, Toddlers Need To Be Vaccinated For Herd Immunity (SN)
Despite what Fauci says, the children don’t actually need the Covid vaccines, as a little fact checking will show. Miniscule benefit to them, compared to significant risks to them from the vaccines. Long-term risks of the Covid vaccines haven’t even been assessed yet, and children have most of their lives still ahead of them.
A recent article in Slate, among others, contradicts Fauci.
“Your 9-Year-Old Is Already Basically a Vaccinated Adult”
How families should think about risk in the final act of the pandemic.The other thing we’re learning more about over time is the directions of spread. So for example, there was a study last week which didn’t get that much attention, of schools in New York. In the cases where they could identify an index case in the small number of what seemed like in-school transmissions, 80% of it involved a staff member. And so there was very little student to student spread. That’s reassuring as we move into the spring, because a lot of those people are being vaccinated. Once you shut off that method, then you’re really talking about a very low risk environment. The only kind of possibility is kid to kid spread. We know that’s not happening much at all. And if it does, those kids are themselves very low risk. So I think you should feel good about it.
The big goal of vaccines is to reduce serious illness and death. That’s what we’re trying to produce with our vaccination. The vaccines we have take a huge risk of hospitalization and death for older adults and reduce it by 85, 95%. Just really big reductions in risk.
The thing is that your 9- or 10-year-old is already basically a vaccinated adult from that standpoint. I mean, it’s true. If you think about the reduction in hospitalization or death risk from being 10, rather than being 80, it’s 99.9%, 98%. It’s actually better than the Pfizer vaccine. I’m hoping that may be a helpful way for people to think about the relative risk for kids, because I think we’ve gotten to this space where it’s like, OK, well, until my kids are vaccinated, I can’t let them out. You’re letting the grandparents out. Let your kids out….
As people, it’s hard to shrink this to the right risk size because of our inability to do small probabilities.
We need to be able to think of COVID like grocery store sushi or something.
Yeah. Just accept, like, sometimes you get it. For kids, especially, it’s a cold. And ultimately with vaccines it’s a cold for the rest of us. And we get those a lot from our kids and other people.
Although not this year.
Right. If you look at pediatric flu deaths, typically that’s about 200 a year. This flu season there was one in the US.
Wow.
One pediatric flu death.
slate.com/human-interest/2021/03/children-and-covid-transmission-your-child-is-basically-a-vaccinated-adult.html
ParticipantMore and more “breakthrough” cases, where people are fully-vaccinated and still become infected with Covid-19, are coming to light. Here’s an example involving four people in the same family.
What are being called “breakthrough” cases of COVID-19 are popping up across the U.S. They’re people who test positive 14 days or more after receiving their last dose of the vaccine…
The 27-year-old’s vaccination card shows she received her second dose of the Pfizer vaccine on January 12. She said she found out she was positive on March 18 from one of the routine tests she takes weekly for work. Believing it might be a false positive, Rewerts said she took a rapid test, which also came back positive.
She said her mother and two other family members – all fully vaccinated – also tested positive this week. They are experiencing symptoms.
Meanwhile, a recent study evaluated the mRNA vaccines from Pfizer and Moderna for effectiveness against 10 strains of the Covid virus that are currently circulating. For 5 of the 10 strains, the vaccines failed. The mutations were “highly resistant to neutralization.”
The vaccines were formulated last year to fight the older strains. The vaccine designs “were finalized early in the pandemic and based on the sequence of the first-reported virus from Wuhan, China. Given the global scale and magnitude of the ongoing pandemic, including case reports of re-infection, it is clear that viral evolution will continue.”
The proposed solution: more vaccines, as boosters.
Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity
https://www.medrxiv.org/content/10.1101/2021.02.14.21251704v2.fullParticipantThis sounds ominous.
Global Ethical Considerations Regarding Mandatory Vaccination in Children
JulianSavulescu PhD, AlbertoGiubilini PhD, MargieDanchinPhD
The Journal of Pediatrics
20 January 2021Whether children should be vaccinated against coronavirus disease-2019 (COVID-19) (or other infectious diseases such as influenza) and whether some degree of coercion should be exercised by the state to ensure high uptake depends, among other things, on the safety and efficacy of the vaccine. For COVID-19, these factors are currently unknown for children, with unanswered questions also on children’s role in the transmission of the virus, the extent to which the vaccine will decrease transmission, and the expected benefit (if any) to the child.
Ultimately, deciding whether to recommend that children receive a novel vaccine for a disease that is not a major threat to them, or to mandate the vaccine, requires precise information on the risks, including disease severity and vaccine safety and effectiveness, a comparative evaluation of the alternatives, and the levels of coercion associated with each. However, the decision also requires balancing self-interest with duty to others, and liberty with usefulness…
Mandatory vaccination for children might be required if vaccine uptake will not be high enough or if governments have reasonable grounds to believe so…
Mandatory vaccination means that some form of coercion is used to get people to vaccinate themselves and/or their children. Vaccine mandates are fundamentally about restricting individual or parental liberty for the public good or for a child’s own good. Coercion means that threats of penalties are used to restrict a person’s options, by making certain options (eg, vaccine refusal for oneself or for one’s child) significantly more costly….
Coercion restricts liberty by narrowing the range of options reasonably available to people…
The restriction of liberty should only be considered when the problem is significant and there is a large expected harm of not intervening. This happens, for instance, when a life-threatening virus like COVID-19 is circulating at high levels in the community…
The relevant question is whether the expected public health benefit of vaccinating children is large enough to justify an intervention on children that might not be overall beneficial for them…
Given the relative uncertainties around the COVID-19 vaccine, it will be difficult to justify mandatory vaccination in children, at least initially.
https://www.sciencedirect.com/science/article/pii/S0022347621000287
ParticipantHow can the Covid vaccine trials on infants and children be considered ethical? Setting aside the informed consent issue, the benefits to children are minimal, while the potential risks to these children are substantial.
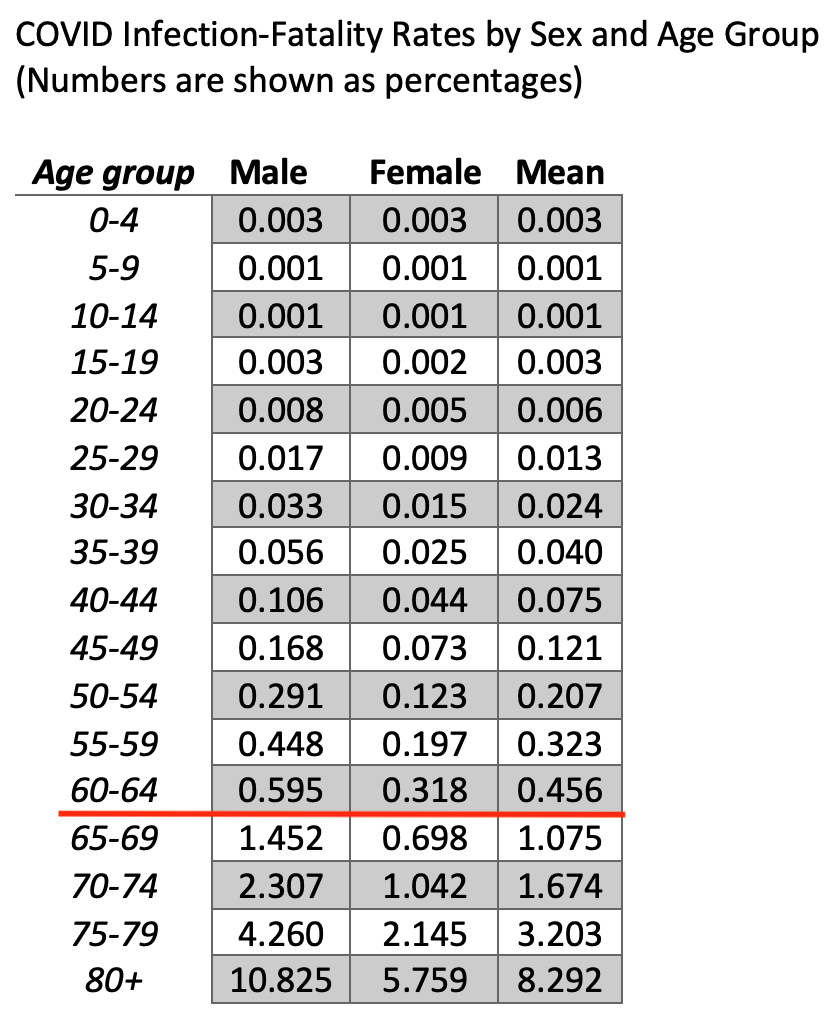
The above chart (if it posted) shows that the Infection Fatality Rate (IFR) for those under age 20 is only 3 (or less) deaths per 100,000 infections. The IFR doesn’t reach 100 per 100,000 (or 1 death per 1,000 infections) until age 45-49. It jumps up to 1,000 deaths per 100,000 infections (1%) in ages 65-69, increasing to 3,000 per 100,000 (3%) for ages 75-79.
The vaccine might make sense for someone in the 75-79 age group who is scared of a 3% fatality rate, but people of that age are literally 1000 times more likely to die from Covid than somebody under age 20 (according to that chart).
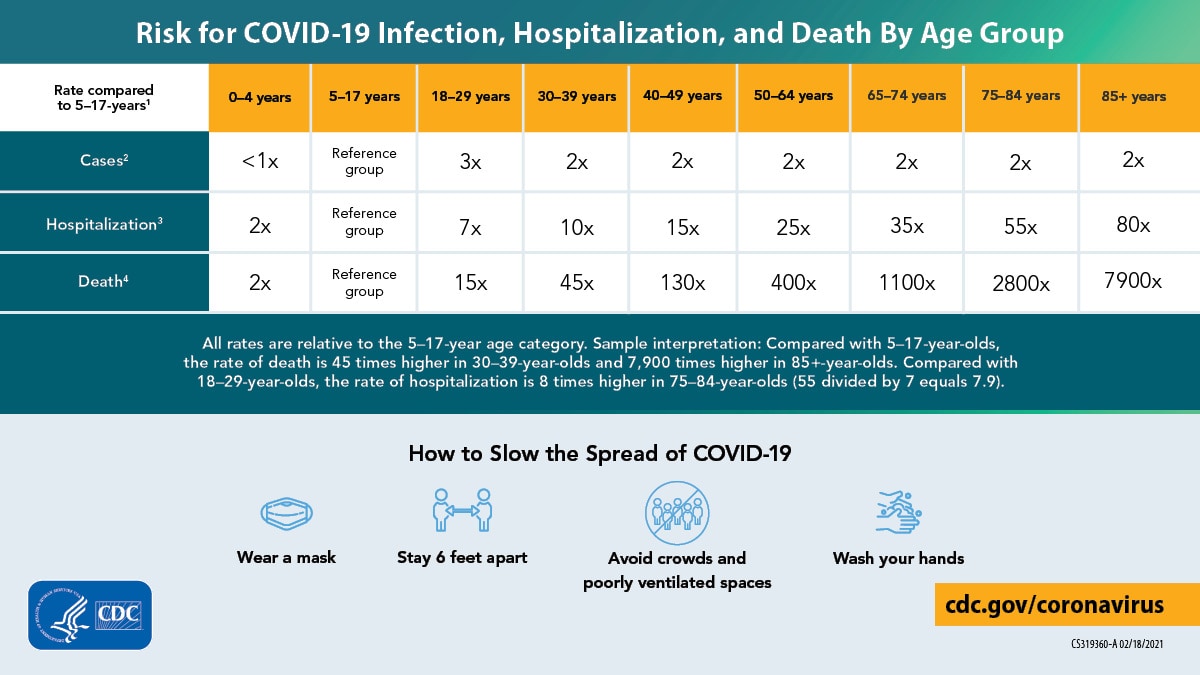
The CDC has published similar data.
Risk for COVID-19 Infection, Hospitalization, and Death By Age Group
“Compared with 5—17-year-olds, the rate of death is 45 times higher in 30—39-year-olds, [2,800 times higher in 75—84-year-olds,] and 7,900 times higher in 85+-year-olds.“
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.htmlThe vaccine benefit/risk judgement call for oldsters is much different that for youngsters, since the risk to oldsters is thousands of times higher, while the long-term risks of the experimental vaccine are much higher for the youngsters (who have their whole lives ahead of them).
ParticipantA handy graphic from the CDC showing how the risk of Covid death for oldsters, and thus the potential benefits of an effective vaccine, are thousands of times greater than for youngsters.
 Participant
ParticipantClarification to my earlier comment:
The vaccine benefit/risk judgement call for oldsters is much different that for youngsters, since the Covid risk for oldsters and the corresponding benefit of the vaccine is thousands of times higher for the oldsters, while the long-term risks of the experimental vaccine are much higher for the youngsters (who have their whole lives ahead of them).
ParticipantThe chart which wouldn’t post in my above comment…
COVID Infection Fatality Rates by Age Group
(Numbers are shown as percentages)
e.g., 0.003 = 0.003% = 3 per 100,000…can be found at this page:
https://www.acsh.org/news/2020/11/18/covid-infection-fatality-rates-sex-and-age-15163ParticipantHow can the Covid vaccine trials on infants and children be considered ethical? Setting aside the informed consent issue, the benefits to children are minimal, while the potential risks to these children are substantial.
The above chart (deleted because it wouldn’t post) shows that the Infection Fatality Rate (IFR) for those under age 20 is only 3 (or less) deaths per 100,000 infections. The IFR doesn’t reach 100 per 100,000 (or 1 death per 1,000 infections) until age 45-49. It jumps up to 1,000 deaths per 100,000 infections (1%) in ages 65-69, increasing to 3,000 per 100,000 (3%) for ages 75-79.
The vaccine might make sense for someone in the 75-79 age group who is scared of a 3% fatality rate, but people of that age are literally 1000 times more likely to die from Covid than somebody under age 20 (according to that chart).
The CDC has published similar data.
Risk for COVID-19 Infection, Hospitalization, and Death By Age Group
“Compared with 5—17-year-olds, the rate of death is 45 times higher in 30—39-year-olds, [2,800 times higher in 75—84-year-olds,] and 7,900 times higher in 85+-year-olds.“
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.htmlThe vaccine benefit/risk judgement call for oldsters is much different that for youngsters, since the risk to oldsters is thousands of times higher, while the long-term risks of the experimental vaccine are much higher for the youngsters (who have their whole lives ahead of them).
ParticipantThe latest data on excess deaths in Europe (for week 10, 2021) was released today. The total weekly excess deaths, from all causes, are again below the baseline (below zero) for every age category.
Looking at the map, all of the reporting countries are showing “No excess” deaths in Week 10 except for Estonia, Netherlands, and Israel (“moderate” excess, one step above “low” excess.)
The media has lots of coverage about Israel’s success with the vaccines, but I haven’t seen any news coverage about why Israel’s excess deaths are higher than all those countries in Europe.
https://www.euromomo.eu/graphs-and-maps#excess-mortality
(choose Weekly instead of Cumulated)Participant• Past Covid Infections Don’t Confer Strong Enough Immunity (F.)
The study results suggest that previous infection gives “a protection rate against reinfection of 80.5%.” This is right up there with the effectiveness of vaccines, maybe even higher when considering the variants.
“Don’t Confer Strong Enough Immunity” is the slant to fit the narrative.
Meanwhile, there are increasing cases where Covid Vaccines Don’t Confer Strong Enough Immunity.
From the Hawai’i State Department of Health, March 11
The Department of Health also recently identified a case of COVID-19 in a fully vaccinated Hawai‘i healthcare worker which was associated with recent travel to the mainland United States. An Oahu healthcare worker received two doses of an approved COVID-19 vaccine in accordance with recommended vaccine guidelines, completing the vaccine series in early January 2021. The individual then traveled to multiple mainland U.S. cities approximately one month later. Pre-travel testing was performed for the individual and a travel companion in preparation for returning to Hawai‘i. Results were received after the travelers arrived back in Hawai’i; both individuals tested positive.
The next day, March 12, “The Hawaii Department of Health (DOH) has announced three cases in which a fully vaccinated person contracted COVID-19. The DOH said, fully vaccinated means the person received both doses of the Moderna and/or Pfizer vaccine.”
www. khon2.com/coronavirus/doh-confirms-3-vaccinated-hawaii-residents-tested-positive-for-covid-19/This can’t just be happening in Hawaii. Are the other states suppressing the news of vaccinated people catching Covid?
Participant“The Curious Case of Geert Vanden Bossche”
When I read Dr. Bossche’s article (posted at TAE), it struck me that his proposed solution would “require large vaccination campaigns” using “NK [natural killer] cell based vaccines,” yet he didn’t give details about this type of vaccine.
I later learned, from his LinkedIn page, that he was the inventor of “a new vaccine technology”, and he is the founder of a company called Univac, which aims to use his invention to create “a new type of vaccines” based on Natural Killer cells.
“I founded Univac as inventor of a new vaccine technology which I subsequently further developed as CSO of the Company. The technology enables the development of universal vaccines educating the host immune system to redirect immune targeting away from canonical antigens to a widely divergent spectrum of vitally vulnerable pathogen-derived ‘self-mimicking’ antigens, irrespective of MHC polymorphism. Although ‘non-self’ and exposed on the surface of infected or pathologically altered cells, these antigens are not effectively recognised upon natural infection or disease.
This new type of vaccines harnesses the power of the immune system by unlocking the untapped potential of self-centered Natural Killer (NK) cells capable of recognising these unconventional antigens.”
https://be.linkedin.com/in/geertvandenbossche
In my view, his credibility went way down because of the self-promotion and publicity for his company which underlies his article.
ParticipantV. Arnold: “100 brands of oat products all came up positive for glyphosate. There are organic oats that have tested free of glyphosate, but do not know which ones”
Those lab results:
https://cdn3.ewg.org/sites/default/files/u352/EWG_Glyphosate-2_Table_Full_C02.pdfThe “365” brand of “old-fashioned rolled oats” had ND (none detected). There are other brands of organically-grown rolled oats, not tested here, which claim to be “Glysophate-Free” (such as Country Life Natural Foods).
ParticipantHuskynut: “The NZ house price article is pay-walled so I couldn;t read it”
I appreciate hearing your views from NZ.
I used DuckDuckGo to search for the headline, and found the entire article, no paywall:
https://consumersadvisory.com/2021/03/14/by-targeting-house-prices-new-zealand-shows-the-way/ParticipantThis journal article echoes what commenters VietnamVet and V. Arnold (among others) have been saying.
Is living in the US conducive to your health?
Chris Fradkin, Current Research in Behavioral Sciences, 6 March 2021In numerous health markers, the United States is low ranking, compared to other high-income nations. Regarding Covid-19 management, the performance of the United States has been abysmal, compared to other nations… Living in the US is not conducive to our health. In fact, the environment is more threatening than that of any OECD nation. Until the US reconfigures its core values, through reduction of disparities in wealth, there will be no future other than the one that is before us, which according to the experts is bleak.
https://www.sciencedirect.com/science/article/pii/S2666518221000176
March 12, 2021 at 12:39 am in reply to: Mass Vaccination Amidst A Pandemic Creates An Irrepressible Monster #70989ParticipantIn other words, “the science” says that the immune escape/evasion problem with current Covid vaccines means that masking and physical distancing will have to continue, and even redoubled, not relaxed. This is the opposite of what Dr Fauci and the CDC are now recommending.
Geert Vanden Bossche, on the other hand, proposes a different kind of vaccine rollout, which will strengthen the body’s Natural Killer cell response to all Covid variants, while reducing the propensity for the Covid virus to mutate to these more dangerous variants.
March 12, 2021 at 12:19 am in reply to: Mass Vaccination Amidst A Pandemic Creates An Irrepressible Monster #70988Participant“Our study and the new clinical trial data show that the virus is traveling in a direction that is causing it to escape from our current vaccines and therapies that are directed against the viral spike… Such considerations require that we stop virus transmission as quickly as is feasible, by redoubling our mitigation measures and by expediting vaccine rollout.”
In that article, the lead author of the study (published in Nature) confirms that “immune escape” is a problem, but his proposed “required” solution is to fully commit to these vaccines, and redouble (not relax) masking and physical distancing (and lockdowns?)
“We have to stop the virus from replicating and that means rolling out vaccine faster and sticking to our mitigation measures like masking and physical distancing. Stopping the spread of the virus will stop the development of further mutations.”
The authors of the Lancet article (linked earlier) propose a different solution which essentially rules out continued general lockdowns and calls for governments to “apply available measures in a way that is much more targeted to different generational groups,” such as self-isolation of “the older and more vulnerable groups” to reduce their risk of infection.
Participant• 2 Separate Studies Debunk Theory That Vitamin D Protects Against Covid-19 (RT)
RT’s coverage of those 2 studies is even worse than The Guardian.
“Vitamin D supplements may offer no Covid benefits, data suggests” (The Guardian)March 11, 2021 at 4:14 pm in reply to: Mass Vaccination Amidst A Pandemic Creates An Irrepressible Monster #70961ParticipantThis article published in The Lancet similarly addresses the problem of “immune evasion.” It calls for an end to “fear-based approaches based on seemingly haphazard stop-start generalised confinement as the main response to the pandemic; approaches which expect citizens to wait patiently until intensive care units are re-enforced, full vaccination is achieved, and herd immunity is reached.”
Dealing with immune evasion will require a re-evaluation of public health strategies…
If substantial immune evasion occurs, current vaccines are likely to still offer some benefit to individuals. At the population level, however, they could induce viral selection and escape, making the prospect of achieving herd immunity increasingly remote.
This virological game changer has numerous consequences, not only for vaccines and treatment, but also for prevention and control strategies. The fervently awaited end of this global health crisis might be continually postponed, as new variants emerge and immune evasion reduces vaccination effectiveness in the short and medium term.
Hence, it is time to abandon fear-based approaches based on seemingly haphazard stop-start generalised confinement as the main response to the pandemic; approaches which expect citizens to wait patiently until intensive care units are re-enforced, full vaccination is achieved, and herd immunity is reached.
Populations have so far been relatively complacent, but their doubts and distrust are visible in protest movements in several countries. The impact of general confinement on entire economies has been devastating, with worse still to come in levels of unemployment and national debt. Social and health (including mental health) consequences are also colossal, in particular for the younger generations, despite them being at low risk in terms of morbidity and mortality from SARS-CoV-2 infection.
https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(21)00036-0/fulltext
March 11, 2021 at 3:40 pm in reply to: Mass Vaccination Amidst A Pandemic Creates An Irrepressible Monster #70957ParticipantA related article:
Tuberculosis vaccine may help protect against COVID-19Scientists developed the BCG (bacillus Calmette-Guérin) vaccine more than 100 years ago to protect against the bacterial infection tuberculosis (TB). According to the World Health Organization (WHO), by 2004, around 100 million children a year were receiving the vaccine…
Scientists believe the vaccine primes the “innate” immune system, the body’s first line of defense against viruses and other invading organisms. Unlike adaptive immunity, innate immunity rarely targets specific pathogens that the body has encountered in the past…
In August 2020, Medical News Today reported another observational study, which suggested countries with mandatory BCG vaccination had a degree of “herd immunity” against the disease.
There are 22 clinical trials currently investigating BCG’s potential to prevent or treat COVID-19, which should provide more definitive evidence.
https://www.medicalnewstoday.com/articles/tuberculosis-vaccine-may-help-protect-against-covid-19
March 11, 2021 at 3:39 pm in reply to: Mass Vaccination Amidst A Pandemic Creates An Irrepressible Monster #70956ParticipantA summary of the problem, using quotes from above:
“We are currently turning vaccinees into asymptomatic carriers shedding infectious variants.”
“Basically, we’ll very soon be confronted with a super-infectious virus that completely resists our most precious defense mechanism: The human immune system.”A summary of the proposed solution, using quotes from above:
“Natural Killer] NK cell-based vaccines will primarily enable our natural immunity to be better prepared (memory!) and to induce herd immunity (which is exactly the opposite of what current Covid-19 vaccines do as those increasingly turn vaccine recipients into asymptomatic carriers who are shedding virus).”Which vaccines result in more NK cells? The BCG vaccine sounds promising against Covid-19 (and it’s been safely used for more than a century.) The OPV and MMR vaccines may also be promising.
From the Journal of Clinical Investigation:
Through the epigenetic and metabolic reprograming of innate immune cells, particularly monocytes, macrophages, and NK cells, BCG vaccination induces a long-lasting memory and the capacity to respond more strongly upon restimulation (17). This nonspecific boosting of the innate immune response following BCG vaccination has also been reported for other live, attenuated vaccines, including the OPV (19) and MMR (20) vaccines. Indeed, studies have shown that both OPV and MMR vaccines are associated with a decreased number of hospital admissions for infections, including fewer respiratory tract infections (37–39). Therefore, in addition to BCG vaccination, OPV or MMR vaccination may also be considered to mitigate the SARS-CoV-2 pandemic until safe and effective COVID-19–specific vaccines become available.
…Taken together, these results indicate that a history of BCG vaccination confers a nonspecific protective effect against SARS-CoV-2 infection and is associated with fewer self-reports of COVID-19 symptoms.
ParticipantMore like an undergrad statistics project, instead of a high school project.
ParticipantRe: Vitamin D article in the Guardian
The first study cited by the Guardian doesn’t apply to people with a Vitamin D deficiency, as noted above.
The other study cited by the Guardian is on shaky ground, as it used aggregate data for Covid mortalities and recoveries (obtained online from Worldometer) and estimations of overall prevalence of Vitamin D deficiencies in various countries (from mention they found in unrelated studies on PubMed.) It sounds like a high school level project. In my opinion, it doesn’t really address whether the Vitamin D deficient people in those countries would get improved Covid outcomes after taking Vitamin D supplements. The study admits that their findings are “not in line with outcomes of similar research works published recently.”
https://www.medrxiv.org/content/10.1101/2021.03.04.21252885v1.full.pdf
Participantisland raider: “Vaccine adverse event reporting from the US CDC website…”
A more comprehensive view of the data can be found at this site, using the VAERS data once it’s made public. These are the results as of 2/26/2021:
From the 2/26/2021 release of VAERS data:
Found 25,212 cases where Vaccine is COVID19Death 1,265 5.02% [of reports)
Permanent Disability 479 1.9%
Office Visit 3,888 15.42%
Emergency Room 22 0.09%
Emergency Doctor/Room 4,908 19.47%
Hospitalized 2,742 10.88%
Hospitalized, Prolonged 1 0%
Recovered 9,236 36.63%
Birth Defect 36 0.14%
Life Threatening 886 3.51%
Not Serious 8,946 35.48%(Because some cases have multiple vaccinations and symptoms, a single case can account for multiple entries in this table. This is the reason why the Total Count is greater than 25212 (the number of cases found), and the Total Percentage is greater than 100.)
https://www.medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUP1=CAT&EVENTS=ON&VAX=COVID19
ParticipantMy above comment wouldn’t post until I divided it into 3 sections.
Here’s the link to the study I quoted:
https://www.medrxiv.org/content/10.1101/2020.09.08.20190975v5.full.pdfParticipantThis bears repeating: That study, which questioned the Covid-related benefits of Vitamin D, did not apply to people having a vitamin D deficiency.
If the Guardian were honest, it would instead report something like “Vitamin D supplements may offer no Covid benefits for those who already have adequate levels of Vitamin D, data suggests”
Followed by reporting on the significant percentage of the population that is indeed deficient in vitamin D.
ParticipantYet, the study which the Guardian uses to support its claim says this:
“our results do not apply to individuals with vitamin D deficiency.”(continued)
ParticipantThat article in the Guardian (linked by chettt) says that “evidence for a direct link between vitamin D deficiency and Covid outcomes is lacking.”
(continued)
Participant• Overweight, Obese Americans Make Up 8 in 10 Covid Hospitalizations (F.)
As I pointed out in a comment above, “Overweight, Obese Americans” make up more than 7 in 10 Americans. The percentage hospitalized for Covid isn’t much different than the percentage in the general population.
However, I looked at the hospitalization data in that CDC report and found:
Americans Over 64 Make Up Nearly 8 in 10 Covid Deaths.A relevant comparison: 16.5% vs 76.5%
Americans age 65 and older are only 16.5% of the population.
Yet, that CDC report shows that 76.5% of the Covid deaths occuring in hospitals were age 65 and older.US population demographics:
https://www.census.gov/quickfacts/fact/table/US/PST045219Participant• Overweight, Obese Americans Make Up 8 in 10 Covid Hospitalizations
This sounds fairly incriminating, at first glance. The “8 in 10,” more accurately stated, is 79.1%.
“Among 148,494 adults who received a COVID-19 diagnosis during an emergency department (ED) or inpatient visit at 238 U.S. hospitals during March–December 2020, 28.3% had overweight and 50.8% had obesity.”
But, hold on. What’s the percentage of the American adult population (in general) that is overweight or obese? 73.6% (in 2017-18, and might be higher for 2020?).
So, 79% of those hospitalized for Covid are obese or overweight, while 74% of the general population is obese or overweight.
79% vs 74% is not as remarkable as the headline might suggest.
Well then, what if we only look at the data for the obese. “One half (50.8%) of adult COVID-19 patients in this analysis had obesity, compared with 43.1% in the total PHD-SR sample and 42.4% nationally.”
If obesity was totally unrelated to the likelihood of being hospitalized with Covid, then we would expect around 42.4% of the hospitalized patients to be obese. The data shows that 50.8% are obese. This is frankly not as big a difference as I expected, based on earlier news coverage.
ParticipantThe CDC admits that this change in policy is being made to get more people to accept the vaccine. They also admit the decison is a judgement call (not simply and strictly following “the science”), where benefits may (or may not) outweigh the risks.
“Additionally, taking steps towards relaxing certain measures for vaccinated persons may help improve COVID-19 vaccine acceptance and uptake.”
-
AuthorPosts