Constantin Brancusi Portrait of George 1911

Last week, Tyler at Zero Hedge ran an article from a site called Adventures in Capitalism, in which the writer (Kuppy?!) lets his light shine on the CIVD19 situation. He concludes that we’re all going to get it, it’s no use resisting, there will never be a vaccine and herd immunity is all we have left to hope for.
And I was thinking: what if he’s -largely- right? What if the utter lack of preparedness and the glaring incompetence we see displayed before our eyes all across the globe has made escape -almost- impossible? Surely at the very least we should prepare for that, too, even if it’s not the only thing we should prepare for.
Not that I’ve strayed much from my original viewpoints, that it’s very dumb to for instance have lengthy discussions about how efficient facemasks and lockdowns are, as long as they’re the only tools you have. But if nobody has a playbook for such things, including the WHO that gets paid millions for exactly that, you do run the risk of making your only tools obsolete.
It’s been a pretty wild year so far what with the spectacle of all the politicians bending like pretzels to avoid being caught unprepared. So many of them have solemnly declared that masks and testing don’t work, simply because they had no access to either. After decades of warnings that a new virus could pop up at any moment.
But you’re right, we now have to look ahead. So first I’ll give you a few “Kuppy” quotes with my comments on them, and we’ll take it from there. Oh, but first this on the morality of a policy aimed at herd immunity, from a BBC piece on the “achievements” of the British gov’t in the virus crisis. “Anthony Costello, professor at University College London and a former director at the WHO, tweeted”:
“Is it ethical to adopt a policy that threatens immediate casualties on the basis of an uncertain future benefit?”
And then we can turn to Kuppy:
[..] had they stopped this thing in Wuhan, we would be right to use a containment approach to COVID-19. Instead, it’s everywhere and despite your personal opinions on the issue, it isn’t going away until most of us get it. There, I said it; you can hide in your basement, but you’re still probably going to get COVID-19. You can quarantine a whole nation; they’ll just get it next year. We are a global economy and this is now a global disease.
Whether you like it or not, the world is going for “herd immunity.” Unfortunately, there is no other viable option; there will be no vaccine, there will be no miracle cure and besides, the virus isn’t even all that dangerous if you are young and healthy. Simply put, COVID-19 won’t flame out until 50 to 80% of us get it (the precise number is open to debate).
I think a lot of people at this point in time would mostly agree with what he says there. But do they oversee the consequences?
Unlike smallpox or polio, there will never be a vaccine (there has never been a COVID vaccine for a variety of reasons)—therefore, as soon as quarantine ends, we’d all begin to spread it again, as there will always be infected humans. Countries that hermetically sealed their borders would not be immune either—they’ve simply deferred infection.
You can quarantine a village in Africa and stop a disease like Ebola that strikes fast and often kills the host. You cannot stop the spread of something that tens of millions of global citizens unknowingly have, while lying dormant for up to three weeks.
More things many would agree with. But will there really always be infected humans, and will they always spread the virus around the entire planet? Is that true? The virus needs new hosts all the time, and if you keep potential hosts sufficiently separated from each other, it can not spread.
We may have a global economy with global citizens, but we’ve seen plenty evidence that what has caused hospitality and travel to plummet has not been lockdowns, but people’s fear of getting infected. Is that irrational, and will you be able to convince them otherwise?
I think it should be obvious that you cannot stop COVID from spreading, at best, you can slow it down so that hospitals do not become overwhelmed. Instead, governments are passing draconian and arbitrary laws that do little to slow the spread, yet destroy businesses and communities.
Hmmm. How exactly would you slow it down without masks and lockdowns? Does it seem like a good idea to bring people together again in offices, elevators, planes, trains, restaurants and bars? Right now it doesn’t appear to make much difference, most people wouldn’t go anyway.
I read today that in the UK, almost half of workers -well, those that still have a job- work from home, whereas that number was 5% before virustime. And now the gov’t wants them all back in the workplace. Think they’ll go as long as the virus is out there?
Millions of jobs, and there come hospitality and travel again, are lost forever. People are afraid. And no, that has little to do with a media fear-porn campaign, though the media are as clueless as the politicians, and it’s a comforting thought to be able to blame them.
[..] putting your head in the sand and hoping COVID-19 goes away is foolish. It is time for everyone to accept the inevitable and figure out what that means for themselves and their countries. The current checker-board approach in the US where each state and even each county takes a different approach—is simply making a mess of things.
People can figure what things may mean without first accepting them as inevitable. Many are doing that right now. But yes, the US has been a mess and still is. It’s too large for a one-size-fits-all approach, especially if that has to be made up on the spot.
But the “leaders”, whether in politics, health care or elsewhere, have a fool-proof take on that: they blame each other. Still, the US debacle is something that has grown over years, decades, it hasn’t suddenly appeared, you just didn’t see it before. And it’s not only the US; the entire rich world has the exact same problem.
Here in Miami Beach; we have a 10pm curfew, we have fines and jail time for not wearing masks in public, bars are closed, restaurants can only have outdoor seating and the beach was closed last weekend. It is not clear what any of these measures actually accomplish if tens of thousands are marching around in protests without masks.
As an aside, the stupidest thing around must be people who wear facemasks outside, unless they’re in close proximity to others. Still, there are gov’ts that demand they do. Closing a beach falls in that same category. Unless people get close together. As for the protests, the most cynical remark I can muster is that at least the rioters cover their faces.

As I made my rounds at some of my favorite restaurants this week, owners finally broke down the brave façade; they confessed that they’re financially bleeding to death. Dozens of prominent restaurants have already shut their doors for good—some of these restaurants have been around for decades and survived multiple economic cycles. If the laws are consistent, you can manage your business—if the government changes the rules every few days to combat a bad cold, what are you supposed to do?
Darn, Kuppy, you were doing just fine, and now you have to bring up the dead “just a bad cold” idea? Read on. It’s not.
I think it is time for everyone globally to finally admit that COVID-19 is here, that we are powerless to stop its spread and that most of us are going to get it. The focus should be on protecting those who are elderly or compromised from a health standpoint. When you start from that framework, you can then think through the consequences and adapt policy appropriately.
We haven’t protected the elderly and health compromised during the lockdowns. What makes you think we will when things are supposed to “return to normal”? We locked up the elderly in the petri dishes we call carehomes, and we let kids and the poor stew in their own misery.
You think we’ve learned something from that? I think when outbreaks flare up again, as they do right now all over Europe, they’re going to isolate the old and the young again, and let the poor rot some more.
If you hope you can protect everyone from it, you’re going to postpone the inevitable, while destroying the economy. Once again, I don’t know what the right approach is, but I know that what’s being done today is asinine. It’s time for global leaders to wake up.
I’m pretty sure that’s what we call a false dichotomy. Lockdowns don’t destroy economies, the virus, and people’s fears of getting infected, plus seeing their loved ones be infected, does. Opening everything up is not going to change that for the better.
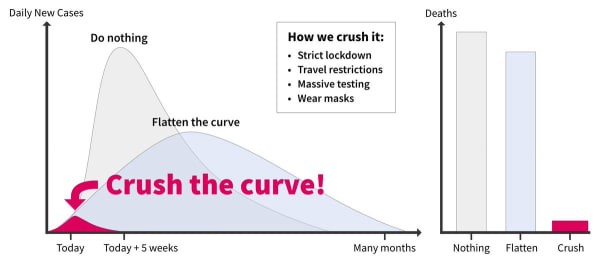
From there it’s just a small step for man and giant leap for mankind towards Kuppy’s only solution left: herd immunity. The idea has already been burned to the ground by numerous parties, but since it’s the only thing he has left, let’s humor him, shall we?
Here’s from a recent BBC piece on the topic, which seems sort of based on the notion that it’s all Britain has left as well. Interesting article though, I must say, they tried to make something out of the whole minestrone :
Did ‘Herd Immunity’ Change The Course Of The Outbreak?
“Herd immunity” is a concept describing the point at which a population has developed protection against a disease. There are two ways to do this. Vaccination is one route. But with any new virus it’s impossible to say how long it will take to develop a vaccine, if ever. The other way is for people to catch the disease and build up some form of immunity. If exposed to the virus again, it is assumed they have protection. If most people in a population are protected then the virus cannot spread.
But there are two problems. One is that with a new virus – like this particular coronavirus – it’s not always clear how much protection having had the disease, particularly a mild case, gives you or how long it lasts. And if most of the population catches the disease, many thousands might die. On 13 March, Sir Patrick stated that about 60% of the population would need to become infected for society to have “herd immunity” – effectively some 40 million people in the UK.
“Communities will become immune to it and that’s going to be an important part of controlling this longer term,” he told Sky News. These comments sparked an immediate backlash. Anthony Costello, professor of health and sustainable development at University College London and a former director of maternal and child health at the WHO, tweeted: “Is it ethical to adopt a policy that threatens immediate casualties on the basis of an uncertain future benefit?”
And from Britain we can go seamlessly to Sweden, perceived as the -internationally heralded- poster child of herd immunity policy, though they never officially endorsed it. A group of 25 Swedish doctors and scientists sounds the alarm on the entire approach, and even suggest it is a “secret goal”.
Sweden Hoped Herd Immunity Would Curb COVID19. Don’t Do What We Did. It’s Not Working.
The motives for the Swedish Public Health Agency’s light-touch approach are somewhat of a mystery. Some other countries that initially used this strategy swiftly abandoned it as the death toll began to increase, opting instead for delayed lockdowns. But Sweden has been faithful to its approach.
Why? Gaining herd immunity, where large numbers of the population (preferably younger) are infected and thereby develop immunity, has not been an official goal of the Swedish Public Health Agency. But it has said immunity in the population could help suppress the spread of the disease, and some agency statements suggest it is the secret goal.
Further evidence of this is that the agency insists on mandatory schooling for young children, the importance of testing has been played down for a long time, the agency refused to acknowledge the importance of asymptomatic spread of the virus (concerningly, it has encouraged those in households with COVID-19 infected individuals to go to work and school) and still refuses to recommend masks in public [..]
Several authorities, including the WHO, have condemned herd immunity as a strategy. “It can lead to a very brutal arithmetic that does not put people and life and suffering at the center of that equation,” Dr. Mike Ryan, executive director of WHO’s Health Emergencies Program, said at a press conference in May.
Regardless of whether herd immunity is a goal or a side effect of the Swedish strategy, how has it worked out? Not so well, according to the agency’s own test results. The proportion of Swedes carrying antibodies is estimated to be under 10%, thus nowhere near herd immunity.
And yet, the Swedish death rate is unnerving. Sweden has a death toll greater than the United States: 556 deaths per million inhabitants, compared with 425, as of July 20.Sweden also has a death toll more than four and a half times greater than that of the other four Nordic countries combined — more than seven times greater per million inhabitants. For a number of weeks, Sweden has been among the top in the world when it comes to current reported deaths per capita. And despite this, the strategy in essence remains the same.
7 months of pandemic without a lockdown, under 10% have antibodies, and the death toll is 7 times that of their neighbors. Something’s not working right?! But Kuppy said it was our only remaining option…
Then again, something that did pique my interest is this very recent development. I could see this concept becoming more potent than any vaccine, if only because as Kuppy rightly notes, there has never been a vaccine for any coronavirus.
New Antibody Mix Could Form ‘Very Potent’ COVID19 Treatment
Researchers have identified a potent cocktail of antibodies that may help doctors treat Covid-19 infections and protect people at risk from falling ill with the disease. The antibodies were collected from patients hospitalised with severe Covid-19, and they could be manufactured at scale by pharmaceutical firms and transfused into the blood to fight the virus or prevent it from taking hold. Scientists at Columbia University in New York screened antibodies from 40 Covid-19 patients and identified 61 types from five individuals that effectively wiped out coronavirus.
Among them were nine that displayed “exquisite potency” for neutralising the pathogen. Tests on cells showed that the antibodies killed off the virus, while experiments with hamsters revealed that an infusion of one of the more potent antibodies protected the animals from disease. “It shut off infectious virus completely in the lung tissue of the hamsters we treated,” said David Ho, a professor of medicine at Columbia who led the research.
[..] Professor Sachdev Sidhu at the University of Toronto also has plans to take neutralising antibodies into clinical trials later this year. “In my opinion, the more antibodies the better, as scaling up antibodies, although standard, still requires time,” he said. “Having multiple options will be good to ensure as many patients as possible can receive the therapies.”
He said every country that is capable of doing so “owes it to their population” to manufacture therapeutic antibodies, and that countries should work together to ensure they can be made available to as many patients as possible at affordable cost.
Then again, antibodies do not come without their own risk. There’s always the risk of a cytokine storm in some form or another. No exception in the case of SARS-CoV-2.
Study Sees Harmful Effect Of Coronavirus Antibodies In ICU
Antibodies generated by the immune system to neutralise the novel coronavirus could cause severe harm or even kill the patient, according to a study by Dutch scientists. Immunoglobulin G (IgG) is a fork-shaped molecule produced by adaptive immune cells to intercept foreign invaders. Each type of IgG targets a specific type of pathogen.
The IgG for Sars-CoV-2, the virus causing Covid-19, fights off the virus by binding with the virus’ unique spike protein to reduce its chance of infecting human cells. They usually appear a week or two after the onset of illness, when the symptoms of most critically-ill patients suddenly get worse. A research team led by Professor Menno de Winther from the University of Amsterdam in the Netherlands said they might have found an important clue that may answer why the IgG appears only when patients are ill enough to be admitted to the intensive care unit (ICU).
The scientists found that the blood from Covid-19 patients struggling for their life on ventilators was highly inflammatory. They observed during a series of experiments that it could trigger an overreaction of the immune system, destroy crucial barriers in tissues and cause water and blood to spill over in the lungs.
It looks like it’s high time, in fact it’s long overdue, that we stop calling COVID19 a respiratory disease. The SARS-CoV-2 virus may enter the body through mouth and nose, but once it’s in, the lungs are merely the first organ it reaches. But it’s through the vascular system that it spreads all through the body.
What we see even in patients that have been declared “recovered”, and we see this time and again, is crippling fatigue, lung damage, heart damage, brain damage, nerve damage, multiple organ damage. And, as a recent report spelled out, blood clotting was found in every organ in the body, including veins, during autopsies.
Many “recovered” patients report symptoms, such as debilitating fatigue, that can last for at least months. We simply don’t know for how long, because it’s only been around for 7 months.
These are things to consider when you say we must surrender to the virus and let it run its course. Even if it doesn’t overwhelm a certain area’s health care system today, we may well be left with huge amounts of people who carry its scars, and need medical assistance, for the rest of their lives.
That appears to be the minimum price you’re going to pay for letting the virus run its course. Is that worth it? Well, not for the girl who’s unlucky enough to catch it, I tell you. For society as a whole then? What’s the price we’re willing to pay for keeping a bar open? I don’t have to answer that question, I only have to ask it. But we as societies do need to come up with an answer.
Is large scale infection inevitable, as Kuppy claims? If so, the consequences look dire. But yes, so do more lockdowns. Agreed. Totally. You tell me. What’s the price you’re willing to pay? A closed bar, a facemask in a store, or a friend’s body crippled for life? You tell me.
To wrap this up, a last study, this one conducted in 69 countries across six continents. I don’t think I’ve seen anything over the past 7 months that I find scarier than this. You see, heart surgery is a life saving procedure for many people, who would be gone without it.
So what happens to your health care system if you let half the population catch the virus, and half of those end up with heart damage in one form or another, to one degree or another? And that’s just the heart, that’s not lungs or brain or nerves or blood vessels.
“55 per cent of patients had an abnormality. One in seven patients were found to have severe abnormalities..”
More Than Half Of All COVID19 Patients Found To Have Damaged Hearts
An international survey of heart scans in people treated for COVID-19 found that 55 per cent of patients had an abnormality. One in seven patients were found to have severe abnormalities. The study adds further evidence to the emerging picture of COVID-19 as a disease of the vascular system in a significant number of cases, and not always primarily a respiratory disease.
It also suggests that a significant of COVID-19 patients will need to be monitored and assessed for permanent damage to the heart. And it raises questions about the extent to which COVID-19 is a disease you may not fully recover from. The research is from a team at the Centre for Cardiovascular Science, University of Edinburgh, UK. They studied echocardiograms from 1216 patients, aged 52 to 71, 70 per cent of them male.
The patients came from 69 countries across six continents. They were all presumed or confirmed cases of COVID-19 when the echocardiograms were taken (between April 3 and April 20, 2020). An echocardiogram uses ultrasound to show how your heart muscle and valves are working. About three-quarters of the patients (901 of them) had no pre-existing cardiac disease. But 46 per cent of their echocardiograms were abnormal, and 13 per cent were found with severe disease.
According to the study: Left and right ventricular abnormalities were reported in 479 (39 per cent) and 397 (33 per cent) patients, respectively. There was evidence of new myocardial infarction in 36 (three per cent), myocarditis in 35 (three per cent), and takotsubo cardiomyopathy in 19 (two per cent). Sixty percent of the scans were performed in an ICU unit or emergency room. About 54 percent of the patients had severe COVID-19. Abnormalities were often “unheralded or severe, and imaging changed management in one-third of patients.”
Study co-author Marc Dweck, consultant cardiologist at the University of Edinburgh, U.K., said in a statement: “COVID-19 is a complex, multi-system disease which can have profound effects on many parts of the body, including the heart. “Many doctors have been hesitant to order echocardiograms for patients with COVID-19 because it’s an added procedure which involves close contact with patients.
“Our work shows that these scans are important—they improved the treatment for a third of patients who received them.” Dr Dweck continued: “Damage to the heart is known to occur in severe flu, but we were surprised to see so many patients with damage to their heart with COVID-19, and so many patients with severe dysfunction.”
Really, you tell me. But don’t tell me only old people die of it. We’re way past that point. And don’t tell me younger people are not affected. That’s like 19th century wisdom. If you want to argue for herd immunity, by all means, but don’t just blurt out something. Let’s see what you got.
I’ve always, as noted before, disliked the wartime, military talk when it comes to this virus, the “we must beat this enemy because it’s out to get us”. This is not the -real- German nazis or the -imaginary- Russians of today. A virus is smaller than you can imagine and it’s not even alive according to science.
But staying with that war talk for a moment, are you sure you want to surrender to it regardless? Or do you want to go with: it’s not that bad, and it’s not that deadly, and those old folk would have died anyway? So open up the bars and everything will be just hunky dory! You sure? Surrender?!
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, your support is now an integral part of the process.
Thank you.
Support the Automatic Earth in virustime.