
Laura Knight The Green Sea, Lamorna 1918

The Automatic Earth’s resident doctor, John Day MD, who’s about to lose his job for refusing to be vaccinated, has compiled a list of OTC prophylactics and treatments for Covid, and specified dosages.
John Day MD: I have gotten a lot of questions from people during the Delta-COVID peak this summer about OTC supplements and repurposed medicines to self-treat COVID, other than staying home alone and awaiting the inevitable, as is routinely advised. All of this advice applies to pregnant women. That is a group with a lot of questions. I am deeply disturbed at how expectant-mothers are being treated by the medical machine these days.
Firstly, don’t use ibuprofen or Aleve. Do not use NSAIDs when sick with COVID-19. I saw information from China in February 2020, and again from France in April 2020 that NSAIDs like these worsened hospital patient outcomes. I don’t know how confirmed that is, nor do I want to await further word. It is easy to avoid them, and they interfere with the anticoagulant effects of aspirin, anyway, which matters, as will be explained.
Support the normal functioning of your immune system with Vitamin-D. Every B-cell and T-cell in your immune system has vitamin-D receptors on it and won’t work properly and intelligently if a lot of them are empty. For most people, in the long term, 5000 units per day of vitamin D-3 (the kind you can buy) is a good dose, and will get people into the normal range. Exceptions to that are people who absorb it poorly and metabolize it poorly. Those people are the ones who still have a low level after months of taking 5000 units per day. You have to do the test to know you need more. People with a lot of body fat distribute their dose into a larger fat volume, and often need more.
A person who has a body weight over 100 kg (220 lb.) might do better to take 10,000 units per day. Checking a blood test after at least 3 months would help confirm what is best. Taking 10,000 units per day for the first month or 2, in order to normalize blood level is good. What is the ideal one time dose of vitamin-D to normalize one’s blood level, assuming a low starting point? A lot of effort has gone into answering that question, and it can be found here:
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC4128480/#R34
Vitamin D3 doses >300,000 IU were similarly effective in patients with 25(OH)D concentrations >20 ng/mL; all 3 studies (29,34,39) observed mean concentrations >30 ng/mL at 4 weeks, though the results peaked at day 3 (reaching 67.1 ± 17.1 ng/mL from 21.7 ± 5.6 at baseline) in the study of Rossini et al (34). Sanders et al (29) showed long-term efficacy of a 500,000 IU dose; the 25(OH)D concentration remained >30 ng/mL at 12 weeks and was significantly increased at 1 year in a cohort of women with osteoporosis.
That dose, 300,000 International Units of vitamin D3, by mouth, corresponds to #60 pills of 5000 units, a month’s worth of taking 2 pills per day. The level peaked at mid-normal in 3 days, and stayed in the normal range at 30 days. An even higher dose, a whole #100 pill bottle of 5000 unit vitamin-D pills produced a 12 week blood level that was still normal. People are very, very reluctant to take that many vitamin-D pills at once, even when they are sick with COVID. I’m sure of that. People give me feedback. “Trust the science”, or something. All I can do is give my best advice, with references.
Here is a flashback to “Vitamin-D Christmas”: https://www.johndayblog.com/2020/12/vitamin-d-christmas.html
Jumping to Z-for-zinc, this paper is the Gospel of Zinc, which has been shown effective against coronavirus “common colds” since 1996, reducing severity and shortening duration of illness. Zinc is clearly good, but it needs to get inside of the cells in order to directly interfere with viral replication. It is nice to have zinc adequacy when you get inoculated with COVID, but you can sure increase your dose when you get a positive test result. In most cases, prophylactic zinc supplementation was more effective than therapeutic proceedings (106–108, 111). Up to 30% of the everyday respiratory infections, briefly named “common cold,” are due to infections with coronaviruses (112).
Studies showed reduced symptom severity, reduced frequency, and duration of the common cold after zinc administration (99, 100, 113, 114) depending on dosage, zinc compound and the start time after initial symptoms (115)…..Zinc supplementation improves the mucociliary clearance, strengthens the integrity of the epithelium, decreases viral replication, preserves antiviral immunity, attenuates the risk of hyper-inflammation, supports anti-oxidative effects and thus reduces lung damage and minimized secondary infections…
https://www.frontiersin.org/articles/10.3389/fimmu.2020.01712/full
What is the optimum preventive-dosing of zinc? The prophylactic dose needs to assure zinc adequacy, without crowding out the absorption of copper. 12 – 25 mg per day seems to be an agreed recommendation. Not exceeding 50 mg/day prophylactically is also broadly agreed. (We get about 12 mg/d in a supplement and eat lots of fresh vegetables.)
What about taking zinc when you are sick with coronavirus? What should be done differently? This gets fancier, and includes quercetin, a plant polyphenol found in foods from onions to green tea. Quercetin acts as a zinc-ionophore and helps zinc get into human cells, including human cells infected with coronavirus, where it inhibits viral production. Taking quercetin together with zinc during active infection has been advised in treatment protocols since at least June 2020, when I first saw it. I was having difficulty prescribing hydroxychloroquine, because of the medical politics which had arisen after President the-Donald had advocated for it.
It was already in fairly wide use by that time. One good thing about HCQ is that it is a zinc ionophore, so I was looking for alternate zinc ionophores, and had heard that quercetin was the main one, especially the available one. I did not get a good idea of how long quercetin persists in the bloodstream after ingestion. That would be expensive to study…
What has been studied is quercetin absorption from the gut, which is poor, but helped by taking it with a meal. It turns out that taking a little lecithin with your quercetin can increase absorption by up to 20 X. They call the mix of 250 mg quercetin + 250 mg sunflower lecithin, in a gel-cap, “Quercetin Phytosome”. We ordered some after seeing this article: Other benefits of quecetin against SARS-CoV-2 are also postulated. They didn’t give zinc, just “quercetin phytosome”.
Results: The results revealed a reduction in frequency and length of hospitalization, in need of non-invasive oxygen therapy, in progression to intensive care units and in number of deaths. The results also confirmed the very high safety profile of quercetin and suggested possible anti-fatigue and pro appetite properties.
https://www.dovepress.com/possible-therapeutic-effects-of-adjuvant-quercetin-supplementation-aga-peer-reviewed-fulltext-article-IJGM
Ground-laying research about the highly-bioavailable formulation, “quercetin phytosome”, mixed with lecithin, and readily available in the retail market.
Quercetin (3,3′ ,4′ ,5,7-pentahydroxyflavone) is a natural flavonoid compound widely found in vegetables, fruits, and nuts. Major dietary sources of quercetin are apple, onions, tomatoes, broccoli, lettuce, and black and green tea… increasing the water solubility of quercetin would enhance its oral bioavailability…
A more soluble formulation of quercetin based on lecithin, Quercetin Phytosome, has recently been developed, and was found to facilitate the attainment of very high plasma levels of quercetin -up to 20 times more than usually obtained following a dose of quercetin- when the novel formulation was administered orally in human volunteers, and it did not have any notable side effects .
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6418071/
COVID has 2 phases , which the Chinese already explained in early 2020. The first week of symptoms (which begins about 5 days after exposure/inoculation) and the second week, where the person either improves with the antibody response the body makes, or gets deathly ill from it. In the second week the battlefield against the virus, and virus-producing cells, lays waste to organs like the lungs, kidneys, blood vessels and heart.
People with inflammatory conditions, like diabetes and obesity, are prone to get hit much harder in the second week. This is the time that people crash fast and get put on high dose steroids and blood thinners in the hospital, to reduce the collateral damage, the “Cytokine Storm”. Those treatments are not over-the-counter. There are some accommodations you can make in anticipation of that. You might decide to take a 325 mg aspirin or two per day, and 1000 mg of vitamin-C three times per day before you get to the second week. The potential benefits outweigh the risks for those with hypertension, diabetes, and obesity..
The more inflammation-prone should take 2 X 325 mg Aspirin per day, to get full benefit of the anticoagulant effect. All the inflammation makes micro clots through the circulation of lungs and kidneys, even brain and heart, and sometimes big clots, too causing overt occlusion of blood supply to heart, lungs and brain.
Vitamin-C has a benefit to cleaning up the oxidative damage and debris where the immune system is fighting the virus, and blasting infected cells with little oxidative-bombs. 1000 mg of vitamin-C 3 times per day is a modest dose in this context. It has been used up to 10X that dose IV in hospital studies last year.
(Astepro). I admit that I am stretching a bit to include this as OTC, but it is approved as such. I would spray it up both nostrils twice per day ASAP.
The 0.15% strength of azelastine nasal spray is now approved for nonprescription treatment of rhinitis – a common allergy to pollens, dust mites, mold and more — in adults and children 6 years of age or older, the agency said. The 0.1% strength remains a prescription product for younger children.
https://www.webmd.com/allergies/news/20210622/fda-approves-first-otc-nasal-spray-for-allergies
Azelastin, hydroxyzine and diphenhydramine were found to inhibit SARS-CoV-2 replication in cell cultures. They are available antihistamines.
Among the three medications, azelastine was found to inhibit the SARS-CoV-2 virus at a dose that was smaller than the amount prescribed as a nasal spray . The other two antihistamines required higher drug concentrations than currently recommended dosing levels to achieve antiviral activity in cells.
https://ufhealth.org/news/2020/existing-antihistamine-drugs-show-effectiveness-against-covid-19-virus-cell-testing
Famotidine (Pepcid) was found to reduce COVID-19 progression, severity and deaths last summer. It likely inhibits cytokine storm effects, but that is not certain. The dose I heard the best reports on was 60 mg 3 times per day, more than cited in the range here: 20-40 mg twice per day should work to full effect..
Impact of Famotidine Use on Clinical Outcomes of Hospitalized Patients With COVID-19
Famotidine use in hospitalized patients with COVID-19 is associated with a lower risk of mortality, lower risk of combined outcome of mortality and intubation, and lower levels of serum markers for severe disease in hospitalized patients with COVID-19…
Famotidine was administered orally in 83% of cases and intravenously in the remaining 17%. Dosing for oral administered famotidine was 20 mg/d in 95.2% of cases and 40 mg/d in the remaining 4.8% of cases. Intravenous famotidine was administered as a 20 mg/2 mL solution in all cases, For inpatient famotidine use, the median total dose was 80 mg (range 40–160 mg) and was received over a median of 4 days (range 2–8 days).
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC7473796/
You might well take 10 mg Zyrtec (cetirizine) twice per day with your Pepcid.
A more recent cohort study used cetirizine and famotidine in hospitalized patients with severe to critical pulmonary symptoms. This study confirmed beneficial reductions in inpatient mortality and symptom progression , probably by minimizing the histamine-mediated cytokine storm
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC7833340/
This article is sparse on details, but the Pepcid + Zyrtec combination might be what they used to treat long-COVID.
Antihistamines might be effective in long-COVID
Regarding therapeutic intervention, almost 60% reduction in symptom burden was observed in long-COVID patients treated with histamine receptor antagonists. Specifically, of 25 patients in the treatment group, 5 reported complete resolution of all symptoms, 13 reported improvements, 6 reported no change, and 1 reported deterioration of symptoms.
https://www.news-medical.net/news/20210608/Antihistamines-might-be-effective-in-long-COVID.aspx
The media, Tony Fauci and the AMA have been beating really hard on ivermectin, the stupid people who use it and the criminals who prescribe it.
Ivermectin is not over the counter in the US.
WARNING : If you take an ivermectin dose to deworm 50 horses, 500 times a typical human dose, you might get sick and die, maybe.
In a trial on human volunteers, doses of 60, 90, and 120 mg were included to establish a significant safety margin for administration of this drug. No central nervous system effects, using pupil size as the parameter, were detected at the maximum dose level. No adverse events were reported in subjects who received 120 mg of ivermectin, which is 10 times the proposed dose of 0.2 mg/kg for treatment of scabies . There was minimal accumulation following multiple dosing (three times per week) with ivermectin, which was consistent with the half-life in the body of about one day.
A safety margin of ten times the recommended dose sounds good, but it gets better. During a program for treating children with scabies in the Solomon Islands, an 8 mg/kg accidental overdose (40 times the recommended dose) in a child caused acute emesis, mydriasis and sedation which rapidly reversed . In a study of poisoning due to ivermectin and the related molecule avermectin,
“Seven patients manifested severe symptoms, such as coma (7), aspiration with respiratory failure (4), and hypotension (3), after a mean ingestion of 100.7 mg/kg avermectin (15.4 mg/kg for ivermectin and 114.9 mg/kg for abamectin). One of the seven patients died, the other six recovered. This was from an average of 500 times the recommended dose rate.
https://wentworthreport.com/ivermectin-safety-profile/
Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8088823/
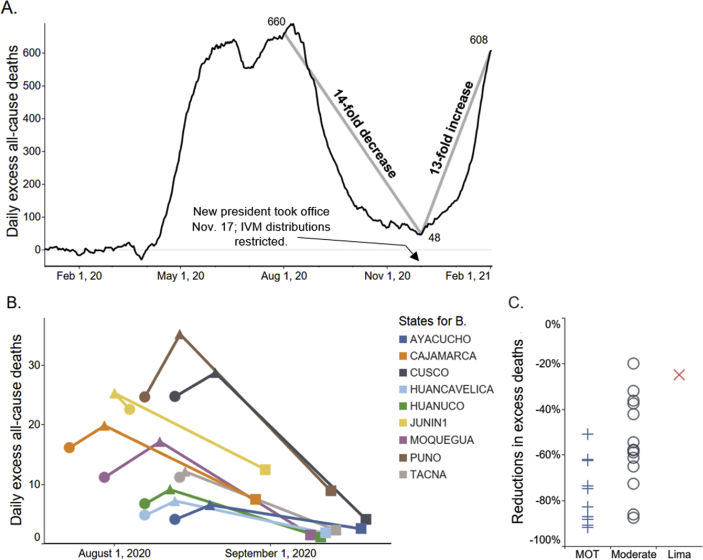
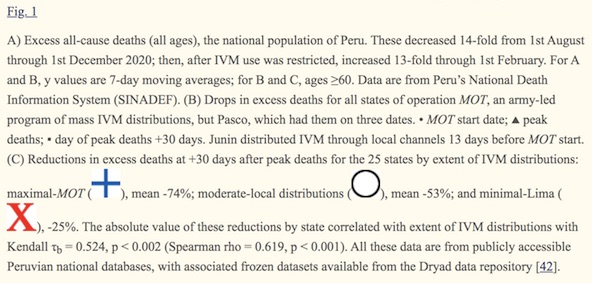
Ivermectin: a multifaceted drug of Nobel prize-honoured distinction with indicated efficacy against a new global scourge, COVID-19 (We wanted to hike Machu Picchu last summer, so I was paying a lot of attention to Peru. The mountainous regions were handing out ivermectin and having very low case counts and deaths, compared to the cities. Last winter Peru got a new president, who outlawed ivermectin. Look what happened:)
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Support the Automatic Earth in virustime. Click at the top of the sidebars to donate with Paypal and Patreon.
