M.C. Escher Fish and Boat 1948

An article by our good- and longtime friend, John Day, family doctor in Texas, until he got canned for refusing the clot shot. Sometimes you think: did that really ever happen? It seems so weird.. But it did, and not that long ago. We lost thousands of qualified and highly capable doctors and nurses for…. well, nothing at all really, other than some people’s petty power games. We lost a lot of lives to those same games too. John looks ahead, rather than back:
John Day:
Western Civilization is at a tense point in history. The current economic arrangements are heavily parasitized, running low on feedstocks like cheap oil, and can’t grow any more, are in irreversible contraction within the current paradigm, legal and bureaucratic structures. The Henry Ford inspired industrial capitalism of the postwar years, where workers could afford the Fords they made, succumbed to the imperative to support the value of the $US, over the actual industrial economy of the US, after America’s vast hoard of gold ran out, draining into the wars in Korea and Vietnam.
In 1971 America’s production of “conventional” oil peaked as previously predicted, and Nixon was forced to default on gold support for the $US, because the gold ran out. The UK got the last of what there was, which was about 40% of what they claimed for the dollars they were handing over.The value of the $US had to be supported somehow. Nixon and Kissinger made the deal with King Faisal of Saudi Arabia, an expansion of the deal FDR made with the Saudis to provide security in return for respecting US/UK interests, and starving the Axis countries. Under the newer deal, the House of Saud could charge any price for oil, but it would be denominated in $US, and excess funds from sales would be invested in US Treasury securities.
The world would need to hold $US to buy oil, supporting the trade-value of the $US. The investment value of the $US also needed to be supported. Interest rates had to be high enough to provide a real return on investment, returning modest, secure profits, whether that was good for the American productive economy or not. After the $US price of oil tripled in the early 1970s, for political-economic reasons (Yom Kippur War, Arab Oil Embargo) there was a corresponding decline of relative $US valuation to that commodity, causing inflation, and a self reinforcing inflationary wage-price rise cycle.
Paul Volcker was appointed Fed. Chairman, as inflation was turning global investors away from the $US as a reserve currency. The dollar suddenly fell from 86% to under 60% of global financial reserves. Volcker raised the interest rates paid on $US (20%) until nobody doubted getting good return on their $US investments, even with inflation. That crushed industry, especially industrial investment, and worker’s wages. No honest man/industry could pay that kind of interest, so borrowing for factories stopped. Financial investments became extractive of real value at high interest rates. Real wages of workers have never again risen from that time. The minimum wage in the US now buys half of what the minimum wage bought in 1968.
This extraction of wealth from workers and industry has supported the value of the $US, and has funded American wars of empire abroad. Government borrowing has funded an increasingly meager form of welfare state within the US. At the same time the productive economy has been made uncompetitive and is increasingly outdated, as the artificially high $US valuation hurt American exports (too expensive) and no honest industry could pay going real rates on investments in US-based production.
Some semi-monopoly industries could be profitable, like aerospace, supported by American military spending. American weapons industries could be profitable, though over time quality fell, while systemic corruption and inefficiencies kept increasing prices. Global customers can now see the price-competitiveness and absolute performance of American weapons-systems in Ukraine. They cn also see how slowly American industry responds to increased demand for supply of munitions during a crisis.
These many decades of paying to support an empire by borrowing and extracting value from the world have hollowed out the value-production chain within the US, and have rewarded parasitic extraction schemes from the productive economy. Hard-squeezed farmers are being strip-mined to support the dollar, but they are now old, and there are just a few of them. America has been sold to investors and rented back to Americans, who are struggling to keep paying rent and bills. Europe is in a similar situation, having taken a somewhat different, but convergent path.
Most nations of the world have had falling prosperity per capita since 2008, or before, due to organizational-complexity, debt, and the rising price of energy products, especially oil. Global “conventional” oil peaked in 2005, causing price rises, and contributing to the 2008 financial crisis (as did other factors). Productive economic growth since then has been minimal, in a system which sees creating a loan and creating a car as equal positives in GDP calculations. Vast borrowing from the future has supported the workings of the system, as investors blithely expect to be paid the promised returns on their loans some day.
“Smart money” is buying real estate, railways, oil and gas wells, power plants and nuclear weapons factories. Manufacturing in countries with low overhead, like Vietnam, Cambodia and Thailand attracts value-investors like China. When the western financial Ponzi scheme breaks down, who will be holding something solid? Will there be competing claims on it? Who will be holding the bag of a lot of unpayable debts? How will this be managed? War is the usual management technique to force cooperation under duress. There are CBDC schemes, Build-Back-Better, Own-nothing-and-be-happy, etc.
The plots to be sprung upon hapless humans appear to be held in waiting while the economic system still works. As corrupt as it is, global economy can still deliver the widest variety of goods, services and real-returns-on-investment ever seen. No gambler can stop while the game is still in play. People who are not “players” can take the initiative to act in this historical moment of pause. Each of us can act historically as we understand the context of the inevitability of crisis and upheaval, and the reason for the calm before the storm.
One might get out of debt and get out of all risk assets, maybe hold physical cash, food, water, propane, a camp-stove, and invest in a safe place in a small town, with mixed local industry, good soil, and a long, peaceful agricultural tradition. Having a good water-well with a solar-powered pump is a remmarkaby practical investment. [I think planning to rely mainly upon firearms is delusional.]
We are social beings. Figure that you will entertain family and maybe friends for extended stays when the financial system breaks down. Understand your regional economic stressors, and how they would flex under duress, like power going out and internet going down, even water, gas and sewer. No trash pick up for a few weeks is something many urban dwellers have experienced. A lot of things morph unexpectedly. How might we live and sustain ourselves in our new economic system? Will the weather try to kill us? Can we devise a low-input lifestyle, and hold a buffer of necessities?
Will forms of civil-war or gang/cartel war come to our area? Is there enough loose wealth to attract those predators? Do we look like prey? There are other strategic forms of initiative which one can take. I had long wondered how to spot the Holocaust, Bolshevik Revolution, Cultural Revolution or “killing fields” early enough to get away in time. We taught our kids about this recurring human pattern. We didn’t know what the definitive sign would be, but I stayed vigilant. When I saw the sign, which was the creation of a human underclass, without rights to bodily autonomy, employment, travel, or even speech, I knew that the dangerous time had arrived.
Paradoxically, I knew that I should not run, but that I should stand firmly and openly as a good example, to help keep history from revisiting the “killing-fields”. All of the historical cases we had studied as a family on our travels had already happened, so our focus looking back was to get away, because we were looking back upon an epoch which DID already happen, and which anybody should have fled.
When the future is uncertain, and you see two directions it might take, you might want to invest with your life or livelihood in the better direction, if you see it clearly enough. All of the other practical investments will serve you in any case, but turning history away from an event where groups of people are dehumanized is always a worthy investment. I wonder what would have happened in Texas if there had not been a significant minority of medical professionals who refused COVID vaccine-mandates and willingly lost their jobs. It was not that many people, but it was public, and selfless and principled, so society did take note. People did discuss it, and it did not just go away.
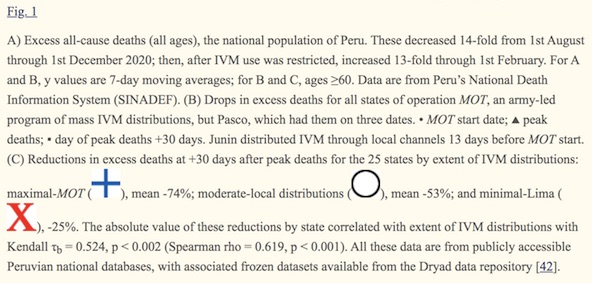
These sacrifices are still being made in the US. Even though the societal-terror has abated, doctors like Pierre Kory MD and Paul Marik MD, who treated people effectively with ivermectin and other life saving therapies, and spread knowledge about how to save lives this way, are now being decertified by their medical specialty boards. The Board of Internal Medicine just decertified them. Their hospitals and the Med Schools where they taught already renounced them to maintain federal funding. The Board of Family Medicine also decertified me early this year, for the same offense of “advising patients against COVID-9 vaccination”. Informed consent for dangerous medical interventions has always been ethically required. “Informed consent” is still legally required, but “I don’t think it means what you think it means”, as the saying goes.
How are we influencing history as it continues to develop and form? Where will our new paths carry us into these uncharted times? Will we look back with regrets? It is hard to know. As it turns out, I am relieved to have avoided the physical harms of the mRNA and viral-vector DNA injections. At the time I had to decide what to do I only thought of myself as not-a-candidate. I did know that ivermectin-based treatment worked very well, especially when started early, which I was prepared to do at home.
You can know yourself to be a historical actor at this pivotal moment. You can act strategically in your own interests, and for your family. You can help friends who will listen, and we can help blaze the historical path which we will trek as a human society.
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.
Support the Automatic Earth in virustime with Paypal, Bitcoin and Patreon.