
Henri Matisse Luxury, calm and pleasure 1904

233
233 New COVID cases apparently…#mainstreammedia #COVID19 #crazy pic.twitter.com/7XY7oY02iz
— ThatDanishGuy (@ThatDanishGuy3) August 10, 2021
China will recognize the Taliban. And then build a pipeline.

Crick
Dr David Bauer
Francis Crick Institute2 doses of Phyza jab lowers neutralising antibodies 5-6 fold.
Essentially it wipes out your immune system making you dependent on booster shots in perpetuity. pic.twitter.com/YTosDnSioP
— Globalist White Papers (@Forest1forTrees) August 13, 2021
Killer T cells
'What we're seeing post vaccine is a drop in your killer T cells, your CD8 cells. And what do CD8 cells do? They keep all other viruses in check.' pic.twitter.com/1UaXOdQz9w
— Consciousness Evolution Movement (CEM) (@coevmo) August 14, 2021
“US intelligence agencies who said just 4 days ago that Kabul could fall in 90 days have revised the figure to 72 hours.”
• Taliban Launches Offensive On Kabul (Sp.)
Biden short
This may become the most infamous — and devastating — press conference ever held by an American President. pic.twitter.com/j4kKwyPDVm
— BDW (@BryanDeanWright) August 15, 2021
The Taliban* has already taken control of all of Afghanistan’s border crossings, leaving the Kabul Airport as the only route out of the country. Taliban insurgents have launched an offensive on Kabul, having surrounded the Afghan capital, the country’s Interior Ministry announced on Sunday. According to the ministry, the terrorists are entering the capital from all sides. The Office of the President of Afghanistan has taken to Twitter to say that the country’s security and defence forces have the situation under control “in coordination with international partners”. The tweet added that gunfire was heard in several remote areas of Kabul. A source told Sputnik that the Taliban had already taken control of Kabul University and raised the group’s flag in one of the city’s districts.
The Associated Press has cited officials, speaking on the condition of anonymity because they weren’t authorised to release the information, as saying there hadn’t been any fighting yet. The insurgents are said to be in the districts of Kalakan, Qarabagh, and Paghman. Less than an hour ago, a member of the negotiating team of the Islamic Republic of Afghanistan, Matin Bek, urged people not to panic and claimed that the Afghan capital was safe. Shortly before the Taliban entered Kabul, the Torkham border crossing with Pakistan, the last post still under the Afghan government’s control, fell to the terrorist group. Thus, the insurgents now control all of Afghanistan’s border crossings. The insurgents took control of the key eastern city of Jalalabad on Sunday, just hours after seizing the northern bastion of Mazar-i-Sharif.
The United States, meanwhile, is sending more troops to the encircled capital to help evacuate its civilians and diplomatic staff as the risk of a Taliban takeover of Kabul became more clear. Earlier this week, US intelligence assessed Kabul could be isolated within 30 days and fall to the Taliban within 90 days.
It’s a neat little trick.
• Defining Away Vaccine Safety Signals (Crawford)
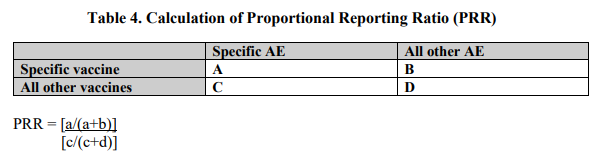
We get to section 2.3, and this is where things get really crazy. This is where signals (for assessing safety/danger of the vaccines) get defined. Subsection 2.3.1 begins (emphasis mine), “CDC will perform PRR data mining on a weekly basis or as needed. PRRs compare the proportion of a specific AE following a specific vaccine versus the proportion of the same AE following receipt of another vaccine (see equation below Table 4). A safety signal is defined as a PRR of at least 2, chi-squared statistic of at least 4, and 3 or more cases of the AE following receipt of the specific vaccine of interest. ” Only a real dork would emphasize the word ‘and’, right? A logic dork, mind you, but we’ll get to that…
First, note that PRR is the proportional reporting ratio, and these PRR numbers are the outputs of a function defined by the CDC based on four variables (which they list in a table as capital letters, then apply in a function as lower-case letters, which always makes me a little uncomfortable as I rarely see such sloppy transition from definitions to application, and somehow they always seem to come from government documentation where I worry about ass covering and plausible deniability).
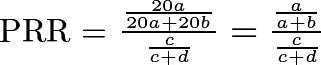
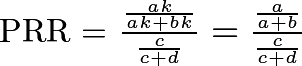
Look at the numerator of this formula. The variables a and b are specific to each vaccine. Now, consider what would happen if an extremely dangerous vaccine were introduced that resulted in 20 times as many AEs of all types as all the other vaccines to which it gets compared.
The PRR remains invariant in the scaling of adverse events!
This means that one vaccine that kills and cripples 20 or 50 or 1,000 times as much as a very safe vaccine will show the same PRR (mild adjustments for variables c and d notwithstanding), and no safety signal will be identified by the CDC. By design. In my circle of discussion, I’ve found out (to my dismay) that this definition of PRR has also been used for other vaccines. Just during the COVID-19 vaccination campaign, important safety signals have come and gone without notice, such as the MedDRA term “death” showed up as a signal in dispersion analysis in February, but no longer does due to the rising quantity of so many other AEs, which forces structural mean-reversion of the PPR function (toward 1) by inflating the denominator. In other words, the number of an AE, a, is normalized to the total number of adverse events (not the number vaccinated, or doses), the ratio of which is then normalized again to the aggregated totals (fraction c over c + d) from other vaccines.
“..there isn’t an aware person who wouldn’t call a halt at this point.”
• Covid-19 Injections Dangerous For Mothers and Babies (Yeadon)
The covid-19 vaccines currently subject to emergency use authorisations all share a common and novel feature: they are gene-based products. Instead of containing a small amount of killed or live-attenuated pathogen, they instead comprise genetic code, instructions as it were to manufacture in our own cells a part of the pathogen. In some products, the genetic code is of DNA & use a weakened respiratory virus to ensure delivery to our cells, or of messenger RNA (the intermediate between the DNA of our genes and the protein product thereby manufactured). There is a further commonality: they cause the recipients cells to manufacture a portion of the SARS-CoV-2 virus called the spike protein. This is literally the spike projecting outwards from the spherical object that contains the virus itself.
As detailed elsewhere in this packet of information, coronavirus spike proteins are biologically active and they initiate the blood coagulation cascade among other properties. It is alleged that it is the induction of blood coagulation in various locations in the body which is responsible for a high proportion of the serious adverse events including deaths which are being reported to the Vaccine Adverse Event Reporting System (VAERS) in the USA and in analogous databases elsewhere. The rate of fatal outcomes following covid-19 vaccination, usually from clotting or bleeding disorders, is extraordinary and exceeds that from any previous vaccine by a very large amount, which this reviewer estimates is of the order of 60-fold.
That this astonishingly high rate of adverse events after vaccination is a consequence of two factors: 1. The manufacturers were simply not required to study the way the product moves around the body after injection and 2. They were not required to study the functional effects of the genetic code within the product after administration. There are no products on the mass market which operate in this way. It is my expert opinion that this is the greatest failure of medicinal product regulation in relation to reproductive health since thalidomide and is very much greater in terms of societal impact. It is imperative that all these products be suspended until improved safety testing can determine whether there are any groups in whom the benefits outweigh the risks.
[..] It is essential to lay out the backdrop to the current position with clinical use of covid-19 vaccines, for one reason: we have NEVER, since thalidomide, exposed women of childbearing potential (WOCBP) and ESPECIALLY NEVER pregnant women to ANY novel, experimental pharmaceutical product without that product first having completed a full battery of reproductive toxicology tests. Even after this crucial step, pilot studies are always conducted in a small number of pregnant women to minimise risk to the developing fetus. Neither of these essential steps have been undertaken.
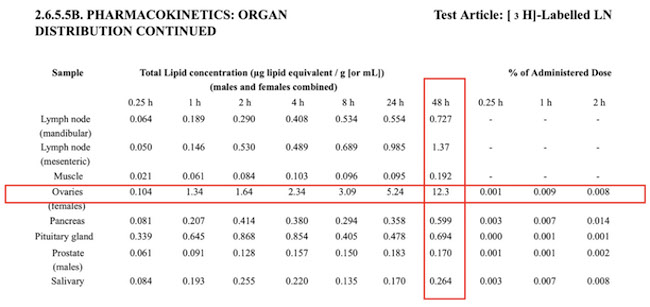
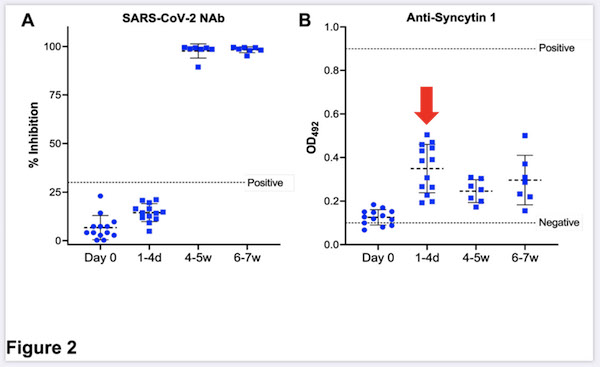
[..] This new data, which shows that women do raise antibodies to a component of their placenta after vaccination with the Pfizer/BioTech product, raises serious concerns for fetal safety. It is not safe to assume that this will not have adverse consequences on successful pregnancy. It is not safe to assume that the other vaccines will not have similar effects. Again, as with the distributional study, a presumption of risk, potentially severe, arises from these clinical observations, and there isn’t an aware person who wouldn’t call a halt at this point.
“There are effective treatments. It’s unnecessary to test asymptomatic people because the CDC says that they don’t spread the virus.”
• Class Action Lawsuit Says Vaccine Has Killed 45,000 People (Rumble)
Michael Green has filed a class action lawsuit at first representing 1,200 first responders against the Governor & Mayor’s vaccine mandates with thousands more expected to join. Michael Green says that the vaccine is killing people all around the country. There are effective treatments. It’s unnecessary to test asymptomatic people because the CDC says that they don’t spread the virus. Honolulu Fire Captain Kaimi Pelekai gives an emotional testimony about losing his job because he doesn’t want to put this experimental vaccine in his body that is killing people.
Mean score drops from 100 to 78.
• Children Born During Pandemic Have Lower IQs (G.)
Children born during the coronavirus pandemic have significantly reduced verbal, motor and overall cognitive performance compared with children born before, a US study suggests. The first few years of a child’s life are critical to their cognitive development. But with Covid-19 triggering the closure of businesses, nurseries, schools and playgrounds, life for infants changed considerably, with parents stressed and stretched as they tried to balance work and childcare. With limited stimulation at home and less interaction with the world outside, pandemic-era children appear to have scored shockingly low on tests designed to assess cognitive development, said lead study author Sean Deoni, associate professor of paediatrics (research) at Brown University.
In the decade preceding the pandemic, the mean IQ score on standardised tests for children aged between three months and three years of age hovered around 100, but for children born during the pandemic that number tumbled to 78, according to the analysis, which is yet to be peer-reviewed. “It’s not subtle by any stretch,” said Deoni. “You don’t typically see things like that, outside of major cognitive disorders.” The study included 672 children from the state of Rhode Island. Of these, 188 were born after July 2020 and 308 were born prior to January 2019, while 176 were born between January 2019 and March 2020. The children included in the study were born full-term, had no developmental disabilities and were mostly white.
Those from lower socioeconomic backgrounds fared worse in the tests, the researchers found. The biggest reason behind the falling scores is likely the lack of stimulation and interaction at home, said Deoni. “Parents are stressed and frazzled … that interaction the child would normally get has decreased substantially.” Whether these lower cognitive scores will have a long-term impact is unclear. In the first few years of life, the foundations for cognition are laid, much like building a house – it’s easier to add rooms or flourishes when you’re building the foundation, Deoni said. “The ability to course-correct becomes smaller, the older that child gets.”
“In mid-December, before the first person had full vaccinated immunity, cases were falling dramatically in the United States. Herd Immunity. For real. It was over. We had suffered, but, had we not been stupid, Covid was more-or-less finished with us.”
“Antibody dependent enhancement (ADE) of infection is a safety concern for vaccine strategies. In a recent publication, Li et al. (Cell 184 :1-17, 2021) have reported that infection-enhancing antibodies directed against the N-terminal domain (NTD) of the SARS-CoV-2 spike protein facilitate virus infection in vitro, but not in vivo. However, this study was performed with the original Wuhan/D614G strain. Since the Covid-19 pandemic is now dominated with Delta variants, we analyzed the interaction of facilitating antibodies with the NTD of these variants. Using molecular modelling approaches, we show that enhancing antibodies have a higher affinity for Delta variants than for Wuhan/D614G NTDs.
We show that enhancing antibodies reinforce the binding of the spike trimer to the host cell membrane by clamping the NTD to lipid raft microdomains. This stabilizing mechanism may facilitate the conformational change that induces the demasking of the receptor binding domain. As the NTD is also targeted by neutralizing antibodies, our data suggest that the balance between neutralizing and facilitating antibodies in vaccinated individuals is in favor of neutralization for the original Wuhan/D614G strain. However, in the case of the Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity. Thus, ADE may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors).”
You stupid, stupid bastards….. Coronaviruses have a long history of doing this sort of thing and its one of the reasons we’ve never managed to have a vaccine developed for them before; it simply doesn’t work. But we were sure it wouldn’t happen this time. It had happened all the other times, but not this time. We were so sure we didn’t need to take the several years required to prove it. We’re smart! We have the new technology, never before deployed in man or beast, which we were absolutely certain would evade the risk that had always, in previous trials, derailed attempted vaccines. Oh, and there were also billions of dollars involved for the companies involved and many newly minted billionaires to be, including the NIH itself who holds some of the patents involved.
So here’s what happened. In mid-December, before the first person had full vaccinated immunity, cases were falling dramatically in the United States. Herd Immunity. For real. It was over. We had suffered, but, had we not been stupid, Covid was more-or-less finished with us. Yes, there were and would remain some of us who hadn’t gotten it, and the extremely rare person who could get it a second time, that would continue to get the virus. It was, however, over. But we were stupid. We jabbed a huge percentage of our population. And as has occurred every other time with coronavirus vaccine attempts the virus mutated around the protection and in fact used the vaccine antibodies to enhance infection. Delta is in fact promoted by those who were vaccinated. As with all other Covid variants most people get a mild or no real illness, but some people get hammered.
However, prior infection doesn’t help if you got jabbed since you took a drug that helps the virus attack you. We created a third wave by our own stupidity: Stupidity seen in nation after nation, but only in nations with high vaccine prevalence; Israel, the UK, Iceland and here in the United States. Don’t run the bull**** on me that this isn’t happening: Not only is the science now in on how its happening but Israel and Palestine, two nations literally next door to each with one having near 100% vaccination and the other about 10% could not be more-stark. Palestine is seeing a small uptick in infections while Israel is getting hammered. The “smartest men in the room” screwed not just a nation — bad enough — but an enormously-large part of the world. Including, quite possibly, you. There’s a reason we’ve never attempted to vaccinate against coronaviruses before. THIS IS THE REASON!
Would new vaccines help? Only until the next one.
• French Study Claims ADE Occurring In Delta Variant Infections (TMN)
A new study by French researchers from Aix-Marseille Université has alarmingly found that ADE or antibody dependent enhancement is indeed occurring in infections with the SARS-CoV-2 Delta variant. The study findings were peer reviewed and published in the Journal of Infections. ADE or antibody dependent enhancement (ADE) of infection is a safety concern for vaccine strategies. A misleading earlier study reported that infection-enhancing antibodies directed against the N-terminal domain (NTD) of the SARS-CoV-2 spike protein facilitate virus infection in vitro, but not in vivo. This study however was performed with the original Wuhan/D614G strain. Importantly since the COVID-19 pandemic is now dominated with Delta variants, the study team analyzed the interaction of facilitating antibodies with the NTD of these variants.
Utilizing molecular modeling approaches, the team showed that enhancing antibodies have a higher affinity for Delta variants than for Wuhan/D614G NTDs. The study team demonstrated that enhancing antibodies reinforce the binding of the spike trimer to the host cell membrane by clamping the NTD to lipid raft microdomains. This stabilizing mechanism may facilitate the conformational change that induces the de-masking of the receptor binding domain. As the NTD is also targeted by neutralizing antibodies, the study data suggest that the balance between neutralizing and facilitating antibodies in vaccinated individuals is in favor of neutralization for the original Wuhan/D614G strain. Alarmingly, in the case of the Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity.
Hence antibody dependent enhancement or ADE may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors). Under these circumstances, second generation vaccines with spike protein formulations lacking structurally-conserved ADE-related epitopes should be considered. [..] It should be noted that all current Covid-19 vaccines (either mRNA or viral vectors) are based on the original Wuhan spike sequence. In as much as neutralizing antibodies overwhelm facilitating antibodies, ADE is not a concern. However, the emergence of SARS-CoV-2 variants may tip the scales in favor of infection enhancement. The study’s structural and modeling data suggest that it might be indeed the case for Delta variants. The study team concludes and warns that ADE may occur in individuals receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors) and then exposed to a Delta variant.
But The Science!
• Denmark Abolishes All Corona Measures (FFN)
Danish parliament recently decided in Copenhagen that all Corona measures should be ended from October 1. There will therefore no longer be a mask requirement and the test regime will be abolished. The Danes will then no longer have to provide evidence of whether they are vaccinated or unvaccinated, or whether they have tested positive or negative. All Corona measures are being lifted in view of the increasing incidence figures in Denmark, reported RT Deutsch. Since the beginning of July this value has risen from 31 to 107,2 (as of August 8). At the same time, the upper limits of this Corona indicator has increased significantly. At the same time, the incidence limits are increased significantly: In communities from 300 to 500 infected people within seven days, in the districts from 500 to 1000.
However, the prerequisite is that an increasing number of Covid-19 patients does not overload the health care system. Denmark’s SSI infectious diseases agency said it no longer relied on vaccination to achieve herd immunity in the country. Tyra Grove Krause, the SSI’s acting academic director, said a new wave of infections were expected after people return to work and school at the end of this summer, but it should not be cause for alarm. “It will be more reminiscent of the flu,” Krause said. Overall, the current vaccination rate is just under 58,4 percent of fully vaccinated people in Denmark. In Germany, this value is only slightly lower at 54,5 percent (as of August 8) but vaccine advocates have been persistent in their fear-mongering and pressure on the unvaccinated.
Tyrolean lawyer Dr. Renate Holzeisen, meanwhile strongly recommended that all employers refrain from vaccination pressure or compulsory vaccination, because most of them were “obviously not even aware of the far-reaching legal consequences associated with it”. The fact that the so-called Covid-19 vaccines, according to the official approval documents of the EMA and the European Commission were not developed and approved for the prevention of infection with the SARS-COV-2 virus, but solely to prevent a more severe course of the disease, were conditionally approved for this reason alone, Holzeisen underscored.
The official approval documents therefore show that these substances cannot interrupt the chain of infection because the people treated with them can become infected and thus be infectious. Practice also proves that people who are completely “vaccinated” become infected with the virus and even have the same viral load as “unvaccinated people” as the CDC, among others, has admitted. It is therefore clear that any Covid-19 “compulsory vaccination” actually lacks any justification. All pressure, including moral pressure (alleged act of solidarity with one’s neighbor) is therefore illegal in terms of criminal and liability law based on the official approval documents.
But we knew they were coming?! Why didn’t you prepare?
• New Covid Variants ‘Will Set Us Back A Year’, Experts Warn UK Government (O.)
Ministers are being pressed to reveal what contingency plans are in place to deal with a future Covid variant that evades current vaccines, amid warnings from scientific advisers that such an outcome could set the battle against the pandemic back a year or more. Recent papers produced by the government’s Scientific Advisory Group for Emergencies (Sage) have suggested that the arrival of a variant that evades vaccines is a “realistic possibility”. Sage backed continued work on new vaccines that reduce infection and transmission more than current jabs, the creation of more vaccine-production facilities in the UK and lab-based studies to predict evolution of variants. With the arrival of a new variant seen as one of the main dangers that could intensify the crisis once again, prominent scientific figures stressed the risks.
Prof Graham Medley, a member of Sage and a leader of the government’s Covid modelling group, said it was “clearly something that the planners and scientists should take very seriously as it would put us back a long way”. “It is not that different to the planning that needs to be done between pandemics – a new variant that was able to overcome immunity significantly would be essentially a new virus,” he said. “The advantage would be that we know we can generate vaccines against this virus – and relatively quickly. The disadvantage is that we would be back to the same situation we were in a year ago, depending on how much impact current immunity had against a new variant. Hopefully, evolution is slow, so that new variants arise that are only marginally evasive rather than one big jump.”
Dr Marc Baguelin, from Imperial College’s Covid-19 response team and a member of the government’s SPI-M modelling group, said preventing the importation of variants of concern with “moderate to high immune-escape properties would be critical, as these could lead to future waves orders of magnitude larger than the ones experienced so far”. “It is unlikely that such a new virus evades entirely all immunity from past infection or vaccines,” he said. “Some immunity should remain at least for the most severe outcomes such as death or hospitalisation. We would most likely be able to update the current vaccines to include the emerging strain. “But doing so would take months and means that we might need to reimpose restrictions if there were a significant public health risk. The amount of restrictions would be a political decision and would need to be proportionate with how much this virus would evade current vaccines.”
Not long ago all of it was voluntary. All of it.
• Booster Shots Will ‘Be Obligatory For Trips Abroad And Care Home Staff’ (DM)
Booster jabs are set to be compulsory for travel abroad and care home staff in plans under discussion by Ministers. A source close to the talks about Covid certification told The Mail on Sunday: ‘The assumption is that you will be required to have the most up-to-date health passport. ‘So if the advice is to have a booster six months after your second jab, then that is what you’ll need.’ At the moment, double-jabbed Brits can go to amber list countries without having to quarantine upon their return. Booster vaccines will be compulsory for care home workers once they are rolled out, a senior Government source said. This will add to the legal requirements for care home staff, who from October will have to be double-jabbed to work in the sector, subject to parliamentary approval.
Millions are set to be offered a third jab from September after Health Secretary Sajid Javid announced the roll-out to priority groups. A Minister told the Mail on Sunday the ‘logical’ move will be to make the booster shots a requirement for travel, adding that the most up-to-date Covid certification for travel will become as normal as the need to have a yellow fever jab to enter certain countries. Last night Sir Iain Duncan Smith, the former Conservative leader, said: ‘If I were the Government I would tread carefully on this. Booster jabs will take a while to get to the majority of the travelling public. ‘And there are issues around whether they are necessary – some scientists say that they may not be necessary.’
Meanwhile talks about what booster jabs will mean for domestic certification are still at an early stage within Government. One insider said that, as domestic passports have only been announced for nightclubs, discussions over whether boosters will one day be required for entry are still in ‘very early days’. The Government will make its decision on boosters following final advice from the Joint Committee on Vaccination and Immunisation (JCVI), which is reviewing the scientific evidence on the third jabs. The JCVI previously issued interim advice in June that Brits ‘should be prepared’ for another round of inoculations.
The article doesn’t know whether to agree or not.
• The Teens Who’d Prefer To Catch Covid Than Have The Vaccine (DM)
Trawling through Government Covid statistics might seem like a strange hobby for a 16-year-old. But when he isn’t practising on his guitar, or watching TikTok videos, that’s what Jacob Mellor can be found doing. And thanks to his keen interest in ‘the data’, he has come to a decision – one that could have a profound impact on his own health and that of those around him. Earlier this month, when it was announced that all 16- and 17-year-olds would be offered a Covid jab, Jacob promptly announced he would be opting out. All the evidence, he says, shows this virus is not a threat to him. And so he feels it would be better to catch Covid, and develop natural immunity, than to have a vaccine.
‘From the beginning we’ve been told that this virus didn’t affect kids,’ says Jacob, from Croydon in South London, who attends an independent school. ‘We even had assemblies about it at school, telling us why we shouldn’t worry because it’s just a cold for people my age. ‘So why should I take a vaccine to protect against something I won’t get ill from? Especially when I know there’s a risk involved with having it. The risk is small, I appreciate that, but it’s still there and I can’t get over that.’ Not only does Jacob have no qualms about catching Covid, he is almost looking forward to it. ‘It would be a good thing, in my eyes. I’d build a strong immunity and I wouldn’t have to worry about risks, like I would with the jab,’ he says.
‘Loads of my friends had Covid last year and the worst that happened was that they were stuck in bed for a couple of days. We all see Covid as something we’re not really bothered about. If I get it, it might suck for a few days, but I’ll be immune, so there’s a benefit to me.’ According to Jacob’s mother Sally, her eldest child – who is one of three, with siblings aged 14 and nine – is ‘an independent thinker’ and has been ‘brought up to appreciate the value of natural immunity’. Sally, a 51-year-old creative director for a major retailer, and husband Steve, 49, a recruitment director, haven’t been vaccinated either. ‘I believe in natural immunity, and I’m nervous about the lack of long-term data about the Covid vaccine,’ she adds.
‘We were a family that would be outside in the dirt and around animals, and I told the kids this would protect them from allergies and make sure they could fight off infections. ‘So Jacob has always asked questions when it came to vaccines, from a very young age – like why did he have to have a tetanus booster, for instance – although he did have all his childhood jabs.’ While more than 16,000 of Britain’s 1.5 million 16- and 17-year-olds took up the Government’s offer to get jabbed last weekend, thousands, like Jacob, are not as enthusiastic. The latest Office for National Statistics Covid survey suggests one in ten of them don’t plan to have the vaccine.
“But *NOW* you are the problem. You are guilty. You are an extremist. You didn’t change at all. Something else changed. But notice how the spotlight on what changed is YOU, and not the origin of the change?”
• I Wish To Take A Little Walk With You And Talk, Deliberately, About This (TLR)
Something shifted after the election of Barack H Obama in 2008. Something subtle that was quietly taking place in the background that surfaced just slow enough so that most people didn’t notice. But before getting to that, let’s first just look at the DHS announcement as presented in their words. Look at this small sentence and the worldview it expresses: ..”Such threats are also exacerbated by impacts of the ongoing global pandemic, including grievances over public health safety measures and perceived government restrictions.”.. Notice the word “perceived”? The government imposed mandates, mask and vaccination requirements are only “perceived government restrictions.” In essence, the chains that bind your expressions of liberty and freedom are merely figments of your imagination.
The needle being forced into the arm of federal workers by the Federal Government is only the perception of a forced medical treatment. Your perception of what they are doing is the problem. You must therefore correct your wrong-thoughts to eliminate the wrong perception. Yes, Dear Leader appreciates your compliance. Your reluctance to change your perception is what identifies you as an extremist. Think about that for a moment with your friends and family. The label of Domestic Extremist is applied to the target who is reluctant to change their perception. The target is transparently innocent of any wrongdoing. They are doing, feeling, believing, and ultimately living, exactly the same as they always have…. but something now is different. You are transparently innocent, yet you are now guilty and labeled. This takes our conversation to an inflection point.
When Barack H Obama was elected/installed as the President of the United States, the people in/around him brought forward a new approach. While the U.S. media had always been biased, manipulative and dishonest, there was something more that changed after the installation of The One, the Lightbringer… and it was assisted by the rise of Big Tech and Social Media. The shift coincided with the merge between the intelligence apparatus and the new platforms of social media. The speed of the shift aligned with the speed of technology that was driving communication. Together the intelligence apparatus, the customary U.S. media and Big Tech began testing how far and how fast they could control the outlook of Americans. Historic leftists, progressives, used to justify their own behavior, and the behavior of their tribe through the media.
History is replete with leftist media excusing the behavior of the transparently guilty. The media would create narratives to justify extremism they aligned with. The transparently guilty were excused and defended. We became used to seeing this. However, when traditional media merged in ideology with social media, no longer was they trying to excuse or justify the transparently guilty of accountability; starting around 2011 & 2012 what the new-era attack started to do was falsely accuse the transparently innocent. Together with ideological institutions in government (Obama’s crew ie. DOJ etc.), the customary U.S. media and Big Tech began testing how far and fast they could control the outlook of Americans… to accuse the transparently innocent. The shift was directly proportional to the training, teaching and development of the crew that came with Obama. All classically trained Saul Alinsky followers.
The Harvard police officer (James Crowley), just doing his job…. that led to Henry Louis Gates outrage, that led to the big PR effort and the beer summit. “Never let a crisis go to waste”… All optically and narrative controlled. Then came George Zimmerman, then Darren Wilson, then The Baltimore Six,… all, again, transparently innocent – but the media framework was exactly the opposite. They were able to label the transparently innocent as ‘guilty’, just by controlling information. Skip through the years of numerous examples as the orchestration continued. The manipulative effort is driven by political intent. Take a transparently innocent person and manipulate a narrative to make them guilty Now, pause for a moment and go back to the current DHS announcement.
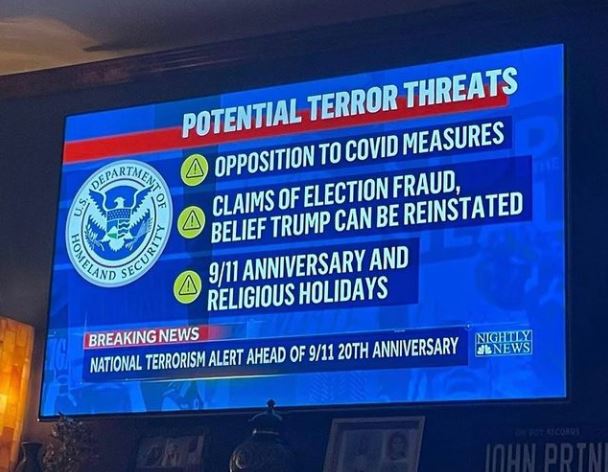
What does this current DHS terrorism bulletin do? It exactly continues the process. Government is now expanding the targeting of the transparently innocent. You hold the same ideas, outlooks, worldviews, and expectations of Liberty and Freedom that you held yesterday, last week, last month and perhaps even long before 9-11-01… But *NOW* you are the problem. You are guilty. You are an extremist. You didn’t change at all. Something else changed. But notice how the spotlight on what changed is YOU, and not the origin of the change? You are the problem. Not those changing the structures of freedom or liberty… YOU are the guilty party. See how they did that? See the shift now?
We try to run the Automatic Earth on donations. Since ad revenue has collapsed, you are now not just a reader, but an integral part of the process that builds this site. Thank you for your support.

Woke Python
For the brilliant woke geniuses at The American Medical Association.
pic.twitter.com/Uf96LtMfe0— TF Metals Report (@TFMetals) August 15, 2021
Mining
— NICO⚡ (@BITVOLT7) August 13, 2021
Support the Automatic Earth in virustime. Click at the top of the sidebars to donate with Paypal and Patreon.

Home › Forums › Debt Rattle August 15 2021