
Doc Robinson
Forum Replies Created
-
AuthorPosts
-
Doc Robinson
ParticipantMore from Peter Doshi, associate editor of the British Medical Journal BMJ:
Let’s put this in perspective.First, a relative risk reduction is being reported, not absolute risk reduction, which appears to be less than 1%.
Second, these results refer to the trials’ primary endpoint of covid-19 of essentially any severity, and importantly not the vaccine’s ability to save lives, nor the ability to prevent infection, nor the efficacy in important subgroups (e.g. frail elderly). Those still remain unknown.
Third, these results reflect a time point relatively soon after vaccination, and we know nothing about vaccine performance at 3, 6, or 12 months, so cannot compare these efficacy numbers against other vaccines like influenza vaccines (which are judged over a season).
Fourth, children, adolescents, and immunocompromised individuals were largely excluded from the trials, so we still lack any data on these important populations.
Pfizer and Moderna’s “95% effective” vaccines—let’s be cautious and first see the full data
https://blogs.bmj.com/bmj/2020/11/26/peter-doshi-pfizer-and-modernas-95-effective-vaccines-lets-be-cautious-and-first-see-the-full-data/Sources of the other quotations from the BMJ:
ParticipantVaccine/antibody ID?
“As a persuasion expert, I keep being asked how to get people to take the COVID vaccine. It’s simple. However, it’s not persuasion, its incentives. Your vaccine/antibody ID lets you go to restaurants, schools, bars, church, fly, or take public transportation, etc.”
“The persuasion that needs to happen is lobbying policy makers and getting public support for COVID ID and incentive policies. You don’t need to persuade everyone, only enough people.“
ParticipantBridge “effectiveness” in that example
= 1 – (44/1000) = 0.956 = 95.6%ParticipantWES: “My bridge is guaranteed @95.6%!”
This means that out of the 165 million people who didn’t use your bridge to get across the water, one thousand of them fell in the water (we don’t know whether they got hurt, or if they only got a little wet), but more than 99.999% of these 165 million people got across the water okay without even getting wet.
Meanwhile, 165 million other people did use your bridge, and 44 of them fell into the water when the bridge failed. We don’t know how badly those people got hurt, either, but because of the experimental materials used to make the bridge, everyone using the bridge has an unknown risk of developing a serious illness, sometime in the future, as a result of crossing the bridge.
In addition, a good proportion of the 165 million people who used the bridge will shortly afterward experience some fatigue, muscle pain, and headache from coming in contact with the experimental materials.
ParticipantBasseterre Kitona: “If we can eliminate 80%o f population from trial studies on that count [already immune], then effectiveness of vaccine in protecting vulnerable people drops to what, something more like 50–75%, right?”
When Pfizer said its vaccine may be “more than 90% effective” this meant that during the vaccine trial, 8 people (out of 20,000) in the vaccinated group became infected, while 86 people (out of 20,000) in the placebo group became infected, giving an effectiveness of 90.7% (based on the relative risk reduction, not the absolute risk reduction).
If 80% of these trial participants were already immune prior to this trial, then the non-immune people would be 20% (or 4,000 in each group), and the “effectiveness” based on relative risk reduction to the non-immune people would still be 90.7%
Imagine a vaccine trial where the entire population of the United States participates, with half the people getting the vaccine and half getting a placebo. If only 86 unvaccinated people (out of 165 million unvaccinated) become infected, while 8 vaccinated people (out of 165 million vaccinated) become infected, then the trial result would still be “more than 90% effective” even though the infection rates are such a tiny percentage of the population.
To me, these are the more relevant numbers coming out of that Pfizer trial:
99.57% of the unvaccinated people did not become infected.
99.96% of the vaccinated people did not become infected.
Absolute risk reduction = 99.96% – 99.57% = 0.39%94 cases in a trial that has enrolled about 40,000 subjects: 8 cases in a vaccine group of 20,000 and 86 cases in a placebo group of 20,000. This yields a Covid-19 attack rate of 0.0004 in the vaccine group and 0.0043 in the placebo group. Relative risk (RR) for vaccination = 0.093, which translates into a “vaccine effectiveness” of 90.7% [100(1-0.093)]. This sounds impressive, but the absolute risk reduction for an individual is only about 0.4% (0.0043-0.0004=0.0039). The Number Needed To Vaccinate (NNTV) = 256 (1/0.0039), which means that to prevent just 1 Covid-19 case 256 individuals must get the vaccine; the other 255 individuals derive no benefit, but are subject to vaccine adverse effects, whatever they may be and whenever we learn about them……We’ve already heard that an early effect of the vaccine is “like a hangover or the flu.” Will vaccinees who are later exposed to coronaviruses have more severe illness as a result of antibody-dependent enhancement of infection (ADEI), a known hazard of coronavirus vaccines? Is there squalene in the Pfizer vaccine? If so, will vaccinees be subject to autoimmune diseases, like Gulf War Syndrome and narcolepsy that have been associated with the adjuvant?
ParticipantupstateNYer: “Excess deaths: if there have been 300,000 in the US to date, that is about 99 people per million (check my math)”
It’s actually more like 900-something people per million (or one out of a thousand people, as I commented above.)
ParticipantI’m going to bypass the testing controversy and look directly at total reported deaths in the US, with a breakdown into cause categories (respiratory, circulatory, alzheimer/dementia, etc.)
A death from respiratory disease (as a category) is relatively easy to determine, without having to know whether it was Covid-19 or not. Looking at it this way gave some surprising results.As a starting point, the overall number of excess deaths (from all causes) is reportedly about 300,000 for this year so far. This amounts to roughly 0.1% of the population (one out of a thousand people), and is roughly 10% of the expected number of annual deaths in the US (based on previous years).
This graph shows the excess deaths for 2020, which can be visualized as roughly 10% of the total deaths for the year:
https://public.tableau.com/profile/dataviz8737#!/vizhome/COVID_excess_mort_withcauses_12022020/WeeklyExcessDeathsWhat types of diseases are causing these excess deaths? The CDC has this data, and it’s not what I expected.
When I look at the most recent data breakdown (published yesterday by the CDC), I find it surprising that since late April of this year, the weekly deaths from respiratory diseases have been about the same as (or less than) the numbers from the previous 5 years.
In fact, respiratory diseases are at most the third highest cause of excess deaths for the year. Circulatory diseases and alzheimer/dementia have the top spots.
https://public.tableau.com/profile/dataviz8737#!/vizhome/COVID_excess_mort_withcauses_12022020/LargeCauseofDeathGroups
(Excess deaths are estimated graphically by the area below the 2020 red line and above the 2015-2019 gray lines average.)Digging deeper within this “Circulatory diseases” category, the two largest causes of excess deaths are “Hypertensive diseases” (high blood pressure) and “Ischemic heart disease” (heart attacks, angina…)
https://public.tableau.com/profile/dataviz8737#!/vizhome/shared/ZW4G68C4B
(Again, the excess deaths are estimated by the area between the red and gray lines. It looks like Hypertensive diseases is the largest cause of excess deaths in this category).This graph brings it all together with “Total number of deaths above average since 2/1/2020, by cause of death”:
https://public.tableau.com/profile/dataviz8737#!/vizhome/COVID_excess_mort_withcauses_12022020/TotalnumberaboveaveragebycauseThe above graph shows that when you look at the “above average” (excessive) deaths, the largest cause is not “Respiratory diseases,” instead it’s “Alzheimer disease and dementia”, and the next highest cause is “Hypertensive diseases”, followed by “Ischemic heart disease.”
All of the “Respiratory diseases” added together into one category are shown to have caused even less “above average” (or “excessive”) deaths than Diabetes caused.
This was surprising and illuminating to me, and I think it puts the situation into better perspective, to say the least.
Participant@ John Day,
I wonder if emailing screenshot images (of the text from your posts) would get past the AI censors?ParticipantDr. D: “We’re claiming a pandemic that has NO ADDITIONAL DEATHS at the end of the year. Yes, early on it pulled a few forward, but now it’s no deaths. Not even among the elderly, as John Hopkins just printed.…Unless you don’t trust John Hopkins.”
I dug deeper into the Johns Hopkins article. It appeared in the Johns Hopkins News-Letter, a student publication. The article was retracted because of a claim that contradicts the CDC data which shows that there have been roughly 300,000 excess deaths (from all causes) in the US this year, compared to the previous 5 years.
Briand was quoted in the article as saying, “All of this points to no evidence that COVID-19 created any excess deaths. Total death numbers are not above normal death numbers.” This claim is incorrect and does not take into account the spike in raw death count from all causes compared to previous years. According to the CDC, there have been almost 300,000 excess deaths due to COVID-19.
https://www.jhunewsletter.com/article/2020/11/a-closer-look-at-u-s-deaths-due-to-covid-19
The article which was retracted:
https://drive.google.com/file/d/1Tnb1a8TXHj_jJCM2BDfGSriUgdn-2gec/viewParticipantSome questions about the effectiveness of the Pfizer and Moderna vaccines, from the British Medical Journal BMJ. The “absolute risk reduction” is relatively small and is being downplayed by the vaccine manufacturers. This is a calculation of how much the vaccine reduces the likelihood that a person would become infected.
For example, if a non-vaccinated person has a 50% chance of becoming infected with a disease, and a vaccinated person has a 10% chance, then the “absolute risk reduction” would be 40%. The absolute risk reductions for the Covid-19 vaccines from Pfizer and Moderna are estimated to be less than 1%.
For the Pfizer vaccine, it’s only about 0.4% reduction. For the Moderna vaccine, it’s only about 0.6% reduction in the risk of having a detectable infection (and less than 0.1% reduction in the risk of getting a “severe” infection).
Thus, for the Moderna vaccine “to prevent one severe illness 1370 individuals must be vaccinated. The other 1369 individuals are not saved from a severe illness, but are subject to vaccine adverse effects, whatever they may be and whenever we learn about them.”
Pfizer’s vaccine “may be more than 90% effective.”
…This sounds impressive, but the absolute risk reduction for an individual is only about 0.4%
…to prevent just 1 Covid-19 case 256 individuals must get the vaccine; the other 255 individuals derive no benefit, but are subject to vaccine adverse effects, whatever they may be and whenever we learn about them……We’ve already heard that an early effect of the vaccine is “like a hangover or the flu.” Will vaccinees who are later exposed to coronaviruses have more severe illness as a result of antibody-dependent enhancement of infection (ADEI), a known hazard of coronavirus vaccines? Is there squalene in the Pfizer vaccine? If so, will vaccinees be subject to autoimmune diseases, like Gulf War Syndrome and narcolepsy that have been associated with the adjuvant?https://www.bmj.com/content/371/bmj.m4347/rr-4
Moderna’s phase III trial has shown that, so far, the vaccine is 94.5% effective. (Mahase, BMJ 2020;371:m4471, November 17) As with the Pfizer vaccine news release, few numbers are provided, but we can approximate the absolute risk reduction for a vaccinated individual and the Number Needed To Vaccinate (NNTV): There were 90 cases of Covid-19 illness in a placebo group of 15,000 (0.006) and 5 cases in a vaccine group of 15,000 (0.00033). This yields an absolute risk reduction of 0.00567 and NNTV = 176 (1/0.00567). There were 11 severe illnesses, all in the placebo group, for an absolute risk reduction of 0.00073 and NNTV = 1370. So to prevent one severe illness 1370 individuals must be vaccinated. The other 1369 individuals are not saved from a severe illness, but are subject to vaccine adverse effects, whatever they may be and whenever we learn about them… Shouldn’t absolute risk reduction be reported so individuals can make fully informed decisions about vaccinations?ParticipantThe other slipper is on the ground, directly below the foot.
https://onartandaesthetics.files.wordpress.com/2016/02/unnamed-file.jpg
ParticipantUK Becomes First Country To Approve Pfizer-BioNTech COVID19 Vaccine
That’s disappointing. A recent editorial in the British Medical Journal bmj says we need more data before an informed decision can be made about the Pfizer and Moderna vaccines.
“…leading both companies to claim around 95% efficacy. Let’s put this in perspective.
First, a relative risk reduction is being reported, not absolute risk reduction, which appears to be less than 1%.
Second, these results refer to the trials’ primary endpoint of covid-19 of essentially any severity, and importantly not the vaccine’s ability to save lives, nor the ability to prevent infection, nor the efficacy in important subgroups (e.g. frail elderly). Those still remain unknown.
Third, these results reflect a time point relatively soon after vaccination, and we know nothing about vaccine performance at 3, 6, or 12 months, so cannot compare these efficacy numbers against other vaccines like influenza vaccines (which are judged over a season).
Fourth, children, adolescents, and immunocompromised individuals were largely excluded from the trials, so we still lack any data on these important populations.
I previously argued that the trials are studying the wrong endpoint, and for an urgent need to correct course and study more important endpoints like prevention of severe disease and transmission in high risk people. Yet…”
Pfizer and Moderna’s “95% effective” vaccines—let’s be cautious and first see the full data
November 26, 2020
https://blogs.bmj.com/bmj/2020/11/26/peter-doshi-pfizer-and-modernas-95-effective-vaccines-lets-be-cautious-and-first-see-the-full-data/ParticipantupstateNYer: “I tried to drill down and finds stats of how many seniors die annually in US nursing homes (long-term care facilities, whichever terminology one chooses). Is 100,000 a lot more than typically die?”
A quick look gave this indication:
“According to previous studies, 20% to 24% of deaths in the United States occur in nursing homes. This number is increasing. [2008]
https://www.jamda.com/article/S1525-8610(08)00172-2/pdf“The total number of deaths in the United States increased from 2.4 million in 2009 to 2.8 million in 2018.”
https://www.prb.org/usdata/indicator/deaths/snapshot/Thus, 20% of 2.8 million = 560,000 deaths (or more) occur in nursing homes during a normal year in the United States (as a ballpark estimate on the low side).
ParticipantThe Russian vaccine EpiVacCorona is based on peptide antigens with an aluminum-containing adjuvant. The carrier protein wasn’t disclosed, but there is speculation that the carrier is a bacterial protein, which would have to be a non-immunogenic type to avoid causing an allergic reaction.
EpiVacCorona (EpiVacCorona vaccine based on peptide antigens for the prevention of COVID-19)
EpiVacCorona vaccine is intended to prevent COVID-19. The vaccine relies on chemically synthesized peptide antigens of SARS-CoV-2 proteins, conjugated to a carrier protein and adsorbed on an aluminum-containing adjuvant (aluminum hydroxide). The EpiVacCorona vaccine contributes to the development of protective immunity against SARS-CoV-2 coronavirus following two intramuscular administrations spaced 21-28 days apart.ParticipantI saw a preprint version of this study earlier this year, and in September it was published in the peer-reviewed journal Environmental Research.
It’s the study which looks at statistics from various locations and calculates the number of miles you’d have to travel per day in a motor vehicle to make the risk of dying from a crash the same as the risk of dying from Covid-19.
Here are some examples of the resulting “risk of COVID-19 death for <65 year old people as miles travelled per day equivalent”:
Canada – 14 miles per day
Italy – 37 miles per day
Netherlands – 32 miles per day
Spain – 65 miles per day
India – 4 miles per dayThis puts the risks into better perspective. The conclusions of the study get straight to the point:
Conclusions
People <65 years old have very small risks of COVID-19 death even in pandemic epicenters and deaths for people <65 years without underlying predisposing conditions are remarkably uncommon. Strategies focusing specifically on protecting high-risk elderly individuals should be considered in managing the pandemic.
Population-level COVID-19 mortality risk for non-elderly individuals overall and for non-elderly individuals without underlying diseases in pandemic epicenters
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7327471/ParticipantCovid-19 official data for Canada, most recent:
https://www.canada.ca/content/dam/phac-aspc/documents/services/diseases/2019-novel-coronavirus-infection/surv-covid19-weekly-epi-update-20201120-eng.pdfIt includes this data regarding outbreak settings, with “long term care and retirement residences” having the most outbreaks, accounting for more than half of Canada’s approx. 12,000 Covid-19 deaths so far.
In second place for number of outbreaks is the “School & Childcare Centre” category, with zero deaths.
https://twitter.com/venivici27/status/1330546719914921986/photo/1ParticipantDr D’s comment seems to be erroneously considering “not for profit” to mean the same as all-volunteer (“work for nothing”).
For example, most community hospitals in the USA are nongovernment “not for profit”, yet employees there can be well paid. CEOs of some nonprofits earn millions of dollars per year.
“The highest-paid nonprofit leaders — CEOs, Executive Directors, etc. — all earn at least $900k per year, and into the tens of millions for the largest of hospitals and health systems.”
https://www.causeiq.com/insights/highest-paid-nonprofit-ceos/
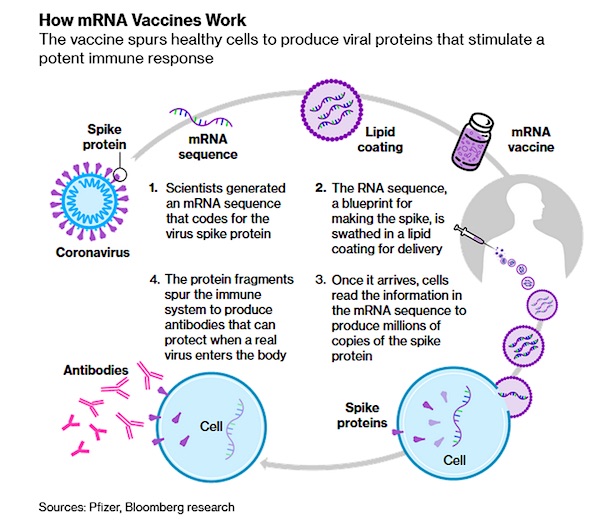
ParticipantFor more information, I recommend this article which was published last month by the American Chemical Society journal ACS Nano. It explains differences and tradeoffs between vaccine approaches, with some companies using a human adenovirus platform (Sputnik V, J&J, CanSino), while others use a chimpanzee adenovirus (Oxford/Astrazeneca). The article also gives details about the nanotechnology involved in the mRNA vaccines, and why some mRNA vaccines may contain chemicals like polyethylene glycol (PEG).

COVID-19 Vaccine Frontrunners and Their Nanotechnology Design
https://pubs.acs.org/doi/10.1021/acsnano.0c07197ParticipantupstateNYer: “how it’s guaranteed that the mRNA…”
I’m not an MD but according to the Jerusalem Post, an article published by the NIH listed some potential risks of mRNA vaccines, including:
1. the bio-distribution and persistence of the induced immunogen expression
[spreading throughout the body and lasting longer than intended]2. possible development of auto-reactive antibodies
[potentially leading to auto-immune conditions]3. toxic effects of any non-native nucleotides and delivery system components.
[such as from nanoparticles and potential allergens like polyethylene glycol (PEG)]But when the world begins inoculating itself with these completely new and revolutionary vaccines, it will know virtually nothing about their long-term effects. “There is a race to get the public vaccinated, so we are willing to take more risks…
But he acknowledged that there are unique and unknown risks to messenger RNA vaccines, including local and systemic inflammatory responses that could lead to autoimmune conditions.
An article published by the National Center for Biotechnology Information, a division of the National Institutes of Health, said other risks include the bio-distribution and persistence of the induced immunogen expression; possible development of auto-reactive antibodies; and toxic effects of any non-native nucleotides and delivery system components.
Could mRNA COVID-19 vaccines be dangerous in the long-term?
https://www.jpost.com/health-science/could-an-mrna-vaccine-be-dangerous-in-the-long-term-649253ParticipantThe vaccines being developed by Russia, J&J and CanSino use a human adenovirus platform, which is a proven technology used in Ebola vaccines and cancer treatments. The other frontrunners are “based on new, largely unproven technology platforms designed to produce vaccines at speed.”
Other vaccine candidates using more conventional approaches won’t have late-stage trial results until sometime in 2021.
I am going to avoid mRNA vaccines like the plague, and wait and see whether the conventional approaches produce anything with a good track record and minimal risk. (I’ve had some vaccines in recent years, but I’ve never had a flu shot.)
Many leading candidates now in final-stage testing are based on new, largely unproven technology platforms designed to produce vaccines at speed.
They include messenger RNA (mRNA) technology used by Moderna Inc and Pfizer Inc with partner BioNTech SE, and inactivated cold virus platforms used by Oxford University/AstraZeneca Plc, Johnson & Johnson and CanSino Biologics, whose vaccine has been approved for military use in China.
Merck & Co in September started testing a COVID-19 vaccine based on a weakened measles virus that delivers genes from the new coronavirus into the body to stimulate an immune response to the coronavirus.
Of these, only the technology offered by J&J and CanSino that use [human] cold viruses as vectors to deliver coronavirus genetic material have ever produced a licensed vaccine – for Ebola. [The Russian vaccine also uses this technology.]
The next set of candidates – with late-stage trial results expected in the first half of 2021 – are heavily skewed toward approaches that have produced successful vaccines.
Conventional methods include using a killed or inactivated version of the pathogen that causes a disease to provoke an immune response, such as those used to make flu, polio and rabies vaccines.
Also more common are protein-based vaccines that use purified pieces of the virus to spur an immune response. Vaccines against whooping cough, or pertussis, and shingles employ this approach.
Next crop of COVID-19 vaccine developers take more traditional route (Reuters)
https://www.reuters.com/article/us-health-coronavirus-vaccine-next/next-crop-of-covid-19-vaccine-developers-take-more-traditional-route-idUKKBN27E0G9ParticipantWhat’s the cost? [Regeneron antibody treatment]
I was wondering that, too. $1,500 per dose, with the first 300,000 doses “free” to patients (paid for by the US government). But it will take the hamsters until the end of January to make those 300,000 doses, while “the nation is approaching 200,000 new coronavirus cases each day.”
“Regeneron’s covid-19 drug is manufactured in cells from genetically engineered hamsters… Unlike conventional pills, these drugs are synthesized by living organisms in specialized reactors, at a biological pace that can’t be rushed.”
https://www.washingtonpost.com/health/2020/11/21/regeneron-fda-clearance/“Regeneron now expects to have REGEN-COV2 treatment doses ready for approximately 80,000 patients by the end of November, approximately 200,000 patients by the first week of January, and approximately 300,000 patients in total by the end of January 2021.”
https://www.prnewswire.com/news-releases/regenerons-regen-cov2-is-first-antibody-cocktail-for-covid-19-to-receive-fda-emergency-use-authorization-301178464.htmlParticipantThe nationalinterest link from zerosum gives these interesting downsides to mRNA vaccines (like Moderna and Pfizer/BioNTech)
as they only allow a fragment of the virus to be made, they may prompt a poor protective immune response, meaning multiple boosters may be needed
there’s a theoretical probability vaccine DNA can integrate into your genome.
ParticipantCovid-19 vaccine side effects?
This summer, Luke Hutchison, a Massachusetts Institute of Technology–educated computational biologist, volunteered for a trial of Moderna’s COVID-19 vaccine. After he got the second injection, his arm immediately swelled up to the size of a “goose egg,” Hutchison says. He can’t be sure he got the vaccine and not a placebo, but within a few hours, the healthy then-43-year-old was beset by bone and muscle aches and a 38.9°C fever that felt, he says, “unbearable.” “I started shaking. I had cold and hot rushes,” he says. “I was sitting by the phone all night long thinking: ‘Should I call 911?’”
Hutchison’s symptoms resolved after 12 hours. But, he says, “Nobody prepared me for the severity of this.” He says the public should be better prepared than he was, because a subset of people may face intense, if transient, side effects, called reactogenicity, from Moderna’s vaccine. Some health experts agree.
“Somebody needs to address the elephant: What about vaccine reactogenicity?…
Fewer than 2% of recipients of the Pfizer and Moderna vaccines developed severe fevers of 39°C to 40°C. But if the companies win U.S. Food and Drug Administration approvals, they’re aiming to supply vaccine to 35 million people in the United States by the end of December. If 2% experienced severe fever, that would be 700,000 people.
Other transient side effects would likely affect even more people. The independent board that conducted the interim analysis of Moderna’s huge trial found that severe side effects included fatigue in 9.7% of participants, muscle pain in 8.9%, joint pain in 5.2%, and headache in 4.5%. For the Pfizer/BioNTech vaccine, the numbers were lower: Severe side effects included fatigue (3.8%) and headache (2%).
That’s a higher rate of severe reactions than people may be accustomed to. “This is higher reactogenicity than is ordinarily seen with most flu vaccines, even the high-dose ones,” says Arnold Monto, an epidemiologist at the University of Michigan School of Public Health.
References about the Russian vaccine (Sputnik V)
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31866-3/fulltext
ParticipantWhat do the Russian vaccine (Sputnik V), the AstraZeneca/Oxford vaccine, the Moderna vaccine, and the Pfizer/BioNTech vaccine all have in common? They all introduce some Covid-19 spike protein genetic material into the body.
The Russian vaccine uses an adenovirus vector (and DNA) to deliver the genetic material. So does the AstraZeneca/Oxford vaccine. “The Russian vaccine is based on two human adenovirus vectors (Ad5 and Ad26), whereas the Oxford vaccine uses a chimp [adenovirus] vector (ChAdOx).”
The Moderna and Pfizer/BioNTech vaccines use mRNA to get the spike protein genetic material into the body. This involves “the use of lipid nanoparticle envelopes to deliver the mRNA cytoplasmically, i.e. directly into the cell.”
Both of these approaches (viral vectors using DNA, and mRNA delivered with lipid nanoparticles) involve some tradeoffs.
Both approaches have had limited success as vaccine platforms, and neither is currently approved for use as a vaccine. They both depend on nucleic acids that encode the target antigen, but differ in their delivery. Viral vectors can enter the cell using viral mechanisms, allowing for high-fidelity production of antigens. However, they can also cause immunogenic responses, or cancers if they adhere to the wrong genes. mRNA delivery depends on the use of lipid nanoparticle envelopes to deliver the mRNA cytoplasmically, i.e. directly into the cell.
LNP [Lipid NanoParticle] delivery is a more novel technique, which currently cannot match the cellular adhesion efficiency of the long-evolved mechanisms employed by viruses. However, once inside the cell mRNA is capable of being directly translated in the cytoplasm, whereas DNA plasmids must be translated via the nucleus back to the cytoplasm. This allows mRNA to produce more antigens from smaller doses, but DNA tends to produce a longer-lasting antigenic effect.
Participant…and the image did not post. Sometimes they don’t.
Participant@ Boogaloo
Here is a sample URL for a JPG image (presented here as a link):
To show this JPG image directly in this comment, I click on the “img” button above the text I’m typing in here, then “enter the URL of the image (previously copied, now pasted here), and I leave it blank where it asks for a description, click on OK and voila:
001.jpg) Participant
Participantchettt: “But Doc, what percent of the population has been tested? Maybe if we tested the entire population the infection rate might just be around 2%”
I don’t know, but if 1% of the swab tests give a false positive, and 1% of the antibody tests give a false positive, then about 2% of people receiving both tests (like the study participants in Denmark) could be counted as infected when they weren’t actually infected.
The current rate of operational false-positive swab tests in the UK is unknown; preliminary estimates show it could be somewhere between 0.8% and 4.0%. This rate could translate into a significant proportion of false-positive results daily due to the current low prevalence of the virus in the UK population, adversely affecting the positive predictive value of the test.
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30453-7/fulltext
We looked for studies that measured the accuracy of antibody tests…
Our findings come mainly from 38 studies..
[Antibody] Tests gave false positive results in 2% of those without COVID-19.ParticipantSomething about that Danish mask study doesn’t add up. The study period ended on 2 June, when there were 11,734 Covid-19 cases in Denmark [Worldometer]. This is only 0.2% of Denmark’s population. Yet the groups in the mask study had infection rates of 1.8% and 2.1% based on the test results.
Could it be that only a very low percentage of the study participants actually became infected during the study, and the reported infections are largely due to false positives from the antibody tests and PCR tests? This could totally explain why both groups had similar results.
Even now, with more than 5 months of new cases added to the total, Denmark’s cumulative number of Covid-19 cases, as a percentage of the population, is only around 1.1%, which is much less than the 1.8% and 2.1% reported for the study participants in June.
Participant@ El Cartero Atomico
That mask study does say “Reported symptoms did not differ between groups during the study period (Supplement Table 3).” And they did antibody tests at 30 days, which could catch the asymptomatic or mild cases.
ParticipantDanish Study Finds Face Masks Provide Limited Protection To Wearer (R.)
That study was done in a place where social distancing and other public health measures were in effect, but masks were not yet recommended, and community use of masks was uncommon.
The study emphasizes that it did not address whether masks are effective as “source control” that protects others.
The study also emphasizes that it did not look at the effectiveness of masks “as protection in settings where social distancing and other public health measures are not in effect.”
The study concludes that the findings were inconclusive.
Our results suggest that the recommendation to wear a surgical mask when outside the home among others did not reduce, at conventional levels of statistical significance, the incidence of SARS-CoV-2 infection in mask wearers in a setting where social distancing and other public health measures were in effect, mask recommendations were not among those measures, and community use of masks was uncommon. Yet, the findings were inconclusive… It is important to emphasize that this trial did not address the effects of masks as source control or as protection in settings where social distancing and other public health measures are not in effect.
ParticipantModerna COVID19 Vaccine Candidate is 94.5% Effective – Trials
mRNA vaccines are “an entirely new technology that hasn’t seen a single approved product.” What could possibly go wrong?
I could see myself maybe getting an mRNA vaccine for something as bad as Ebola, but I think I’ll take my chances by skipping the Covid-19 vaccinations.
ParticipantLockdowns Haven’t Brought Down COVID Mortality, But Killed Millions Of Jobs
Some medical research was published a few days ago, comparing mortality rates for Norway and Sweden. The study looked at mortality rates during the 5 most recent “epidemic years” ending in late July, which covers the vast majority of Covid-19 deaths this year.
These 3 paragraphs from the study are like a breath of fresh air, away from the smokescreens and fear propaganda. I would normally emphasize the important parts of a quotation, but here it’s all good:
Our study shows that although Covid-19 associated mortality rate was almost 15-fold higher in Sweden than in Norway during the epidemic, all-cause mortality was not higher in Sweden compared with three of the four preceding years. An increase in all-cause mortality was only observed in comparison to the immediately preceding period (2018/19), because mortality was lower than in the previous years. The excess mortality was confined to individuals older than 70 years. In contrast, mortality rates were lower than expected for all ages in Norway and individuals younger than 70 years in Sweden.
At the beginning of the Covid-19 epidemic, extensive social measures were introduced in Norway in the form of restrictions and prohibitions to limit the spread of Covid-19 (13–19), while the public health authorities in Sweden chose a much less intrusive strategy (20–25). The Swedish strategy against Covid-19 has therefore received intense international attention and criticism (9), notably because reported mortality rates in Sweden have been higher than in comparable countries such as Norway. In Sweden, however, mortality was lower than expected in the months preceding the epidemic. This finding may suggest mortality displacement.
Mortality displacement (37) entails temporarily increased mortality (called excess mortality) in a population as a result of external events, such as heat waves (38), or epidemics like influenza (39) or Covid-19. The observed temporary excess mortality likely arises because people in vulnerable groups die weeks or months earlier than they would otherwise, due to the timing and severity of the unusual external event. The excess mortality is therefore preceded or followed by periods of lower than expected mortality. The period preceding the excess mortality in Sweden during the Covid-19 epidemic, characterised by lower mortality than usual, might be due, at least partly, to a mild influenza season during the winter of 2019-20 (40). Further, after the Covid-19 epidemic, we might see a decline in morbidity and mortality below normal levels in Sweden, as the oldest and frailest have already died.
Mortality in Norway and Sweden before and after the Covid-19 outbreak: a cohort study
https://www.medrxiv.org/content/10.1101/2020.11.11.20229708v1
https://www.medrxiv.org/content/10.1101/2020.11.11.20229708v1.full.pdfParticipantAnother source confirms “no excess” mortality in Sweden, for their most recent weekly data (Week 44, ending November 1).
ParticipantLet’s look at the graph of Covid cases in Sweden (posted above and copied here for reference):
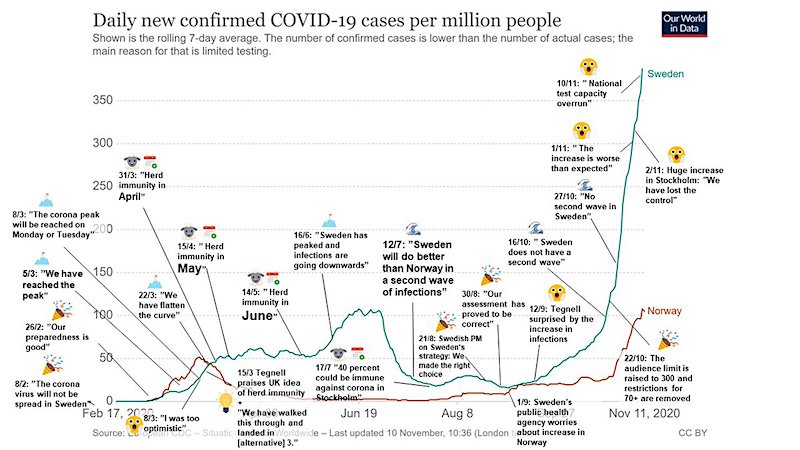
This is not so scary when looking at actual deaths. Excess deaths in Sweden have been negative every week since the end of August (negative meaning less than the average for the past 5 years), according to the same source of the above graph.

https://i.postimg.cc/nVWB9KFq/Excess-Mortality-Covid-Sweden.pngParticipantTypo: 18.3% should be 18.1%.
And those 18% were mostly, by a large margin, people who had a previous psychiatric diagnosis.
“The incidence of any psychiatric diagnosis in the 14 to 90 days after COVID-19 diagnosis was 18.1% including 5.8% that were a first diagnosis.”
ParticipantOne In Five COVID19 Patients Develop Mental Illness Within 90 Days (R.)
I dug deeper into this, because they were including insomnia as a mental illness, when I thought it was a potential symptom of a mental illness, not the illness itself.
The actual study published in the Lancet reveals that “one in five” is really 18.3% (not 20%). For comparison, it would be nice to see how many flu patients similarly develop mental illness within 90 days. The answer appears in Table 3:
Table 3
Estimated incidence of all (first and recurrent) psychiatric diagnoses during the first 14 to 90 days after a diagnosis of COVID-19 compared with other health eventsCOVID-19: 18.1%
Influenza: 13.3%Not so fear-inducing to hear that 13 out of 100 of flu patients develop mental illness (as measured by the study), compared to 18 out of 100 Covid-19 patients.
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(20)30462-4/fulltext
ParticipantDr. D: “This is also what the prospective Q says, who is almost certainly the Trump military intel propaganda wing.”
The latest Honest Government Ad is about Q, and how QAnon is a PsyOp.
“What’s that? When do we take down the Deep State? Oh, honey, the guy who exposed the real Deep State is being tortured by it right now. And where are you? Oh, that’s right. Q told you to trust the plan.”
[Photo of Julian Assange holding The Guardian newspaper with headline “Massive Leak of Secret Files Exposes True Afghan War.]
ParticipantA little more attention to the Assange case, from an article published today:
Peter Oborne, writing last month, issued the call to fellow journalists to take up the case for WikiLeaks. He starts with a scenario: imagine a political dissident held at London’s Belmarsh Prison charged with espionage offences by the People’s Republic of China. The real offence? Exposing atrocities by Chinese troops. “To put it another way, that his real offence was committing the crime of journalism.”
Add to this the findings of the UN Special Rapporteur on Torture that the dissident in question showed “all the symptoms typical for prolonged exposure to psychological torture”, with Beijing pressuring UK authorities to extradite him to a place he could face 175 years in prison. “The outrage from the British press would be deafening.” Protests and vigils outside Belmarsh would be unhalting; debates would take place on “prime time news programmes, alongside a rush of questions in parliament.”
Oborne acknowledges the UK-US alliance. But that should not matter one jot “as far as the British media is concerned.”
https://dissidentvoice.org/2020/10/begging-outrage-british-journalists-for-assange/
Participant“To date, Republicans have turned out 59 percent of their voters in Miami-Dade and Democrats have turned out 53 percent, a 6-point margin. That’s twice the margin Republicans had at this point in 2016..“
That “6-point margin” is misleading when you consider that the number of Democrats in Miami-Dade is 50% higher than the number of Republicans.
If you look at the number of votes already cast by Democrats and Republicans in Miami-Dade, the Democrat number is 35% higher than the Republicans.
Republicans–
59% of 418,661 voters is 247,010 who already voted.Democrats —
53% of 628,412 voters is 333,058 who already voted.https://www.miamidade.gov/global/elections/voter-registration-statistics.page
Participant@ VietnamVet
I’m not finding evidence to support the statement “Long haul symptoms are reported in 25% of the cases.” Instead of 25%, it seems to be more like 2.5%.
A recent study looked at 4,182 cases and found that less than 5% had symptoms lasting more than 8 weeks, and only 2.3% had symptoms lasting longer than 12 weeks. (Long COVID is defined in the Multi-Organ Impairment study as “persistent symptoms three months post-infection.”)
Attributes and predictors of Long-COVID: analysis of COVID cases and their symptoms collected by the Covid Symptoms Study App
https://www.medrxiv.org/content/10.1101/2020.10.19.20214494v1 -
AuthorPosts
