
Doc Robinson
Forum Replies Created
-
AuthorPosts
-
Doc Robinson
ParticipantA study on daily Zinc supplements found that those who didn’t take the Zinc were “7.38 times more likely to develop symptomatic COVID-19 infection as compared with individuals in the treatment group.” This is “equivalent” to having received a vaccine that is 86% effective, according to these calculations:
1 – (1 / 7.38) = 0.86 = 86% effective
Results: Symptomatic COVID-19 infection was significantly higher among the control group participants (N = 9, 10.4%) than the treatment participants (N = 2, 1.9%), p = 0.015. The unadjusted odds ratio indicates that symptomatic COVID-19 infection was 5.93 [95% CI: 1.51, 39.26] higher in the control group, p < 0.01. Controlling for co-morbidities, individuals in the control group were 7.38 (95% CI: 1.80, 50.28) times more likely to develop symptomatic COVID-19 infection as compared with individuals in the treatment group (p < 0.01)…
The findings from our study suggest that zinc supplementation in all three doses (10, 25, and 50 mg) may be an effective prophylaxis of symptomatic COVID-19 and may mitigate the severity of COVID-19 infection.
A Case-Control Study for the Effectiveness of Oral Zinc in the Prevention and Mitigation of COVID-19
https://www.frontiersin.org/articles/10.3389/fmed.2021.756707/fullParticipantMaxwell Quest: “…close friends that still rely on TV media for the pandemic gospel message still beat the vax drum relentlessly.”
That reminds me of something from an article I stumbled upon today:
“In terms of news consumption, only MSNBC and broadcast television act as positive predictors that someone is vaccinated.”Who are the vaccine holdouts? America’s real COVID divide might not be what you think
Are the unvaccinated mostly Republicans, evangelicals and Fox News viewers? I crunched the data: The answer is no
https://www.salon.com/2021/12/22/are-the-vaccine-holdouts-americas-real-divide-might-not-be-what-you-think/ParticipantHeadline from yesterday:
• Justin Trudeau Calls Unvaccinated ‘Racist and Misogynistic Extremists’That nonsense would mean that unvaxxed women are misogynistic extremists, and unvaxxed Blacks are racist extremists.
In Florida, for example, 58% of the White population got a vaxx dose, while 38% of the Black population got a vaxx dose, according to the Latest Data on COVID-19 Vaccinations by Race/Ethnicity (Published: Dec 15, 2021).
Thus, in Florida, 42% of the White population is unvaxxed, while 62% of the Black population is unvaxxed.
Participantzerosum: “Would [the cumulated excess deaths be only lower for the 75-and-older age groups] because the # of [most-vulnerable] 75-and-older age groups are now fewer because the sick etc. have already died ?
That’s my guess. In 2021, the decreased mortality of the 75+ group offsets the increased mortality of the under-75 group, to give an overall decline in excess mortality (for all age groups combined). Looking at all age groups combined like this can be misleading (as in claims that the vaccines lowered excess mortality in 2021), because all the under-75 age groups had significant increases in excess mortality (despite the all-ages excess deaths for the year being lower.)
ParticipantThe stats for Europe’s excess mortality were updated today, and since the end of November, the weekly excess deaths for all age groups have been plummeting. For the cumulated overall year, it looks like 2021 will have less excess deaths than 2020 for all age groups combined. However, when comparing 2021 to 2020 for each age group, the cumulated excess deaths are only lower for the 75-and-older age groups. For every age group under 75, there were more excess deaths (significant increases) in 2021 than in 2020.
ParticipantBoogaloo: “It makes no sense to me to say that a PCR test cannot distinguish a coronavirus from an influenza virus.”
The CDC dropped an earlier PCR test, but it’s currently pushing a PCR test that “can simultaneously detect and differentiate SARS-CoV-2, Influenza A, and Influenza B with one test.”
CDC is recommending that laboratories that routinely conduct influenza testing as well as COVID-19 testing, such as public health laboratories, consider transitioning to a test that can generate a result for both influenza and SARS-CoV-2, rather than running separate tests for each virus. The CDC Influenza SARS-CoV-2 (Flu SC2) Multiplex Assay, one such assay available to public health laboratories, can simultaneously detect and differentiate SARS-CoV-2, Influenza A, and Influenza B with one test. It is a more resource-efficient way for public health laboratories to meet influenza and SARS-CoV-2 surveillance goals.
ParticipantRIM: “Do we know why they withdrew this particular one?”
According to the CDC, their CDC PCR test was the first one available to fill an unmet need in 2020; there are many others available now; and the CDC is retiring this CDC PCR test to focus their resources elsewhere.
Why is CDC retiring the CDC 2019 Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel?
CDC is retiring the CDC 2019 Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel because the U.S. Food and Drug Administration (FDA) has authorized hundreds of other SARS-CoV-2 diagnostic tests, many of which are now higher throughput or can test for more than one illness at a time. At the time CDC deployed the 2019-nCoV Real-Time RT-PCR Diagnostic Panel, there were no other FDA-authorized methods available within the United States.
CDC began distributing the CDC 2019 Novel Coronavirus (2019-nCOV) Real-Time RT-PCR Diagnostic Panel to fill a gap. The wide availability of other SARS-CoV-2 diagnostic tests means that the CDC 2019 Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel is no longer filling an unmet need. Retiring the CDC 2019 Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel will allow CDC to focus its resources on public health surveillance testing and other response activities.
Participant• CDC Admits PCR Tests are Invalid (Martin Armstrong)
Armstrong seems to be reading too much into what the CDC said. The only PCR test being withdrawn is the one that was previously distributed by the CDC, called “the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel.” The CDC started distributing this one in early 2020. There are other brands of RT-PCR tests that are still authorized, available, and not being withdrawn.
Does the retirement of this test apply to all RT-PCR-based tests or all SARS-CoV-2 tests that have received Emergency Use Authorization from FDA?
No. The discontinuation of Emergency Use Authorization (EUA) only applies to the CDC 2019 Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel test.
A long list with other PCR tests that will still be authorized for Covid testing:
https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/in-vitro-diagnostics-euas-molecular-diagnostic-tests-sars-cov-2ParticipantHerrWerner: “…long-term immune dysfunction, long after the virus has passed and been removed from the body, but the spike protein remains”
Reminds me that after the Pfizer injections, spike protein was still found circulating 4 months later.
Circulating exosomes isolated from vaccinated healthy individuals contained SARS-CoV-2 spike protein Ag [Antigen] S2…
Exosomes with spike protein and Abs decreased in parallel after four months… Four months postvaccination, the levels of Ab decreased in plasma. This same trend was observed for circulating exosomes with the spike protein.”
Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer–BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines
https://www.jimmunol.org/content/207/10/2405.longParticipant• Facebook Now Censoring the British Medical Journal (NYNR)
Here’s the primary source, straight from the British Medical Journal BMJ:
Facebook urged to act over incompetent “fact check” of BMJ investigation
https://www.bmj.com/company/newsroom/facebook-urged-to-act-over-incompetent-fact-check-of-bmj-investigation/ParticipantWe don’t need no stinking trials, since “individuals experienced no unusual side effects, meaning that it is likely that a fourth dose would cause no harm either.”
‘Israel could be completely unprotected against COVID-19 in a month’ – report
“Within a month or two, the protection in Israel could be almost back to where it was before vaccines,” reads a report.Israel’s Pandemic Response Team was warned last Tuesday night that Israel could go from being reasonably protected against Omicron to not being protected at all within just a month.
As a result, the team – along with the COVID-19 Vaccination Advisory Board – voted to allow the country’s highest risk population to receive a fourth shot of the Pfizer COVID vaccine, sparking controversy in Israel and around the world.
Health Ministry Director-General Prof. Nachman Ash has still not approved the recommendation – and may not – as more data about the likelihood of developing serious infection from the Omicron variant is starting to emerge.
But why did the committee make a recommendation if it did not have all the data?…the protection afforded people ages 60 and older who received a third dose is expected to decline from 75% to only 25% within a month as the Omicron variant becomes the dominant strain in Israel.
…Regarding safety, the researchers showed that about half a million people had likely recovered from the virus and did not know it, and therefore took three shots of the Pfizer vaccine. These individuals experienced no unusual side effects, meaning that it is likely that a fourth dose would cause no harm either.
https://www.jpost.com/health-and-wellness/coronavirus/article-689749
ParticipantGift ideas:

 Participant
Participant“The end of the pandemic will not be televised”
From the British Medical Journal BMJ, “the covid-19 pandemic will be over when we turn off our screens and decide that other issues are once again worthy of our attention.”
There is no universal definition of the epidemiological parameters of the end of a pandemic. By what metric, then, will we know that it is actually over? The World Health Organization declared the covid-19 pandemic, but who will tell us when it’s over?
The ubiquity of dashboards has helped create a sense that the pandemic will be over when the dashboard indicators all reach either zero (infections, cases, deaths) or 100 (percentage vaccinated). However, respiratory pandemics of the past century show that endings are not clear cut, and that pandemic closure is better understood as occurring with the resumption of social life, not the achievement of specific epidemiological targets…
The notion, reinforced by dashboards, that a pandemic ends when cases or deaths drop to zero is at odds with the historical evidence that substantial influenza morbidity and mortality continues to occur, season after season, between pandemics…
Some historians have observed that pandemics do not conclude when disease transmission ends “but rather when, in the attention of the general public and in the judgment of certain media and political elites who shape that attention, the disease ceases to be newsworthy.” Pandemic dashboards provide endless fuel, ensuring the constant newsworthiness of the covid-19 pandemic, even when the threat is low. In doing so, they might prolong the pandemic by curtailing a sense of closure or a return to pre-pandemic life.
Deactivating or disconnecting ourselves from the dashboards may be the single most powerful action towards ending the pandemic. This is not burying one’s head in the sand. Rather, it is recognising that no single or joint set of dashboard metrics can tell us when the pandemic is over…
Pandemics—at least respiratory viral pandemics—simply do not end in a manner amenable to being displayed on dashboards. Far from a dramatic “end,” pandemics gradually fade as society adjusts to living with the new disease agent and social life returns to normal.
As an extraordinary period in which social life was upturned, the covid-19 pandemic will be over when we turn off our screens and decide that other issues are once again worthy of our attention. Unlike its beginning, the end of the pandemic will not be televised.
The end of the pandemic will not be televised
https://www.bmj.com/content/375/bmj-2021-068094ParticipantAnother notable sentence from “The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory“:
Briefly, although mRNA mainly transfects cells near the injection site, it could hypothetically reach any cell in the body (Maugeri et al., 2019; Pardi et al., 2015).
ParticipantThe latest data from the UK indicates that “THE MORE YOU VACCINATE, the more likely you are to get Omicron.” (The Naked Emperor’s Newsletter).
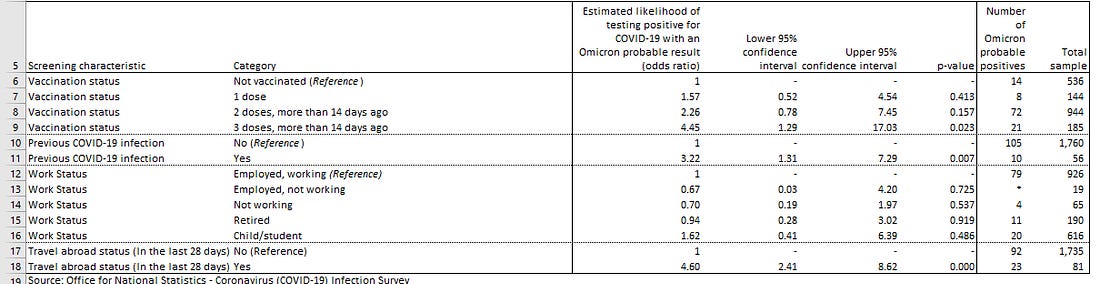
Look at the table above. As the vaccination status increases, the likelihood of testing positive with Omicron increases from 1.57 in one dose individuals, to 2.26 in two dosed and 4.45 in 3 dosed. Due to the small dataset, this is only a modelled likelihood of testing positive with Omicron. This also means the upper and lower confidence intervals are pretty big. However, the upper confidence interval for boosted individuals is 17.03, which is extremely high.
Is this ADE or OAS rearing its ugly head, there is much debate about that online. Is this just a small dataset producing weird results? Maybe but the Danish and Canadian data suggest otherwise.
The New Normal – Pandemics of the Vaccinated?
Are we beginning to see further evidence of ADE or OAS occurring in the UK data?
https://nakedemperor.substack.com/p/the-new-normal-pandemics-of-the-vaccinatedParticipant• US Army Creates Single Vaccine Against All COVID & SARS Variants (Defense One)
Your tax dollars at work (at Ft. Detrick).
The headline is BS.
This line is also BS: “…allows scientists to attach the spikes of multiple coronavirus strains on different faces”. Only one strain is being used in the vaxx, the original Wuhan strain.“Using the initial SARS-CoV-2 genome sequence from Wuhan, China (GenBank: MN9089473), we designed four classes of S-domain ferritin-fusion recombinant proteins as immunogens for expression as nanoparticles based on the major antigenic domains of the S ectodomain (Figure S1). The Helicobacter pylori ferritin molecule was genetically linked to the C-terminal region of the following S antigens: (1) S ectodomain (residues 12–1158)…”
That first design, with “S ectodomain (residues 12–1158)”, is the basis for the Spike-Ferritin-Nanoparticle (SPFN_1B-06-PL) vaxx being used in the clinical trials. It includes the N-terminal domain (NTD) and receptor-binding domain (RBD) of S1, along with S2, “with the spike end residue used to link to ferritin.” The ferritin is bacterial, from H. pylori.
SARS-CoV-2 ferritin nanoparticle vaccines elicit broad SARS coronavirus immunogenicity
https://www.cell.com/cell-reports/fulltext/S2211-1247(21)01639-9Participant• mRNA-LNP Platform’s Lipid Nanoparticle Is Highly Inflammatory (NIH)
That study mentions the long-term presence (after injection in the human body) of the synthetic lipids in the Pfizer vaxx, and how it has not yet been determined whether this could lead to chronic inflammation and “immune exhaustion.”
[FDA Panelist on giving the Pfizer vaxx to 5-year-olds: “We’re Never Going To Learn About How Safe The Vaccine Is Until We Start Giving It”]
The synthetic ionizable lipid in the Pfizer SARS-CoV-2 vaccine has been speculated to have approximately 20–30 days of half-life in humans (Comirnaty, 2021). Whether the long-term presence of ionizable lipid could lead to low levels of chronic inflammation and immune exhaustion (Wherry and Kurachi, 2015) remain to be determined.
ParticipantRIM: “What exactly do we know about Paxlovid and molnupiravir so far? Doc Robinson? Wasn’t molnupiravir 30% effective in one study?
Based on some articles quoted in earlier comments about Paxlovid and Molnupiravir:
Pfizer’s oral treatment Paxlovid combines a very expensive antiviral with a cheap antiviral (Ritonavir). Who knows how much of the benefit is due to the cheap antiviral? (The trials weren’t designed to show this.)
Regarding Merck’s oral treatment Molnupiravir, “the full data show molnupiravir reduced the risk of hospitalization or death for patients with mild or moderate COVID-19 by about 30%.” Almost half of the expert advisors to the FDA voted against the EUA for Molnupiriavir (for high-risk patients), due to the questionable efficacy and safety concerns. (AFAIK, the FDA did not yet grant an EUA to Molnupiravir, but it has already been authorized in the UK.)
More details from my earlier comment about Paxlovid, from November 22:
“Pfizer is conducting a new study with 2634 participants into the efficacy of its PF-07321332 protease inhibitor drug in multi drug combination with HIV drug Ritonavir, against recent Covid-19 infection in the unvaccinated.”
Pfizer’s drug is a very expensive antiviral. Ritonavir is a cheap antiviral.
“Pfizer’s COVID-19 Oral Antiviral Cost $529 per Course… If authorized or approved, PAXLOVID will be administered at a dose of 300mg (two 150mg tablets) of PF-07321332 with one 100mg tablet of ritonavir, given twice daily for five days.”
Pfizer’s drug will be given with the existing antiviral drug Ritonavir which is currently available as a generic at a cost of $3 or less per 100 mg tablet. Pfizer’s clinical trials are comparing the combination of two antivirals (PF-07321332 plus Ritonavir) to a placebo. I think they should be comparing the combination of two antivirals to Ritonavir by itself. Otherwise, how can they know whether PF-07321332 adds a significant benefit above what the existing (and cheap) antiviral Ritonavir would provide by itself?
A Study of PF-07321332/Ritonavir in Nonhospitalized High Risk Adult Participants With COVID-19
More details from my Dec 1 comment about Molnupiravir:
Molnupiravir EUA for high risk adults? Almost half of the experts voted “No” because of questionable efficacy and safety concerns.FDA Panel Narrowly Backs Merck’s COVID Pill
— Questions about efficacy, safety were chief among concerns, regardless of how members votedA divided FDA advisory panel voted 13-10 to recommend the oral antiviral molnupiravir for emergency use authorization (EUA) for adults at high risk of progressing to severe COVID-19 on Tuesday.
While votes at the Antimicrobial Drugs Advisory Committee (AMDAC) were largely split, similar questions were raised on both sides of the vote about modest efficacy, especially in light of other available treatments…
Of particular concern to the “no” voters was not only that efficacy against hospitalization and death declined from the interim analysis submitted to the FDA (48% relative risk reduction) to the final analysis (30% reduction), but that when examining only the data from the post-interim analysis enrollment, there were fewer placebo patients who were hospitalized or died by day 29 versus patients receiving the intervention (4.7% vs 6.2%, respectively)…
For other committee members, potential mutagenicity was an issue, which the committee also discussed, but did not vote on… James Hildreth, MD, PhD, of Meharry Medical College in Nashville, was unequivocal: “It’s an easy vote for me to vote no. Genotoxicity and mutagenicity data raise more questions than answers,” he said…
The FDA does not have to follow the advice of its advisory committees, but it often does.
https://www.medpagetoday.com/infectiousdisease/covid19/95944
From Nov 28:
It turns out that the mutagenic drug Molnupiravir isn’t so effective against Covid.
From Trial Site News:
Merck and Ridgeback Report Full Phase 3 Analysis for Oral Antiviral COVID Pill; Efficacy Plunges from Interim Analysis
The full data show molnupiravir reduced the risk of hospitalization or death for patients with mild or moderate COVID-19 by about 30%, based on a study of more than 1,400 adults. Last month, an interim analysis showed about 50% efficacy, based on data from 775 patients.
So the benefits are less than touted in Merck’s press release, but what about the risks?
Below is a related article in Forbes, by William A. Haseltine (“For nearly two decades, I was a professor at Harvard Medical School and Harvard School of Public Health where I founded two academic research departments, the Division of Biochemical Pharmacology and the Division of Human Retrovirology. I am perhaps most well known for my work on cancer, HIV/AIDS, genomics and, today, on COVID-19.”)
Harming Those Who Receive It: The Dangers Of Molnupiravir (Part 2)
Yesterday I wrote about the potential dangers the antiviral drug molnupiravir could unleash by supercharging new SARS-CoV-2 variants. Today, my focus is on the people who may receive the drug as a treatment and the possibility that molnupiravir could lead to cancerous tumors in those patients and birth defects in the unborn.
Molnupiravir is a relatively new drug, initially developed as an antiviral treatment for influenza…
Participant“A SARS-CoV-2 ferritin nanoparticle vaccine…”
More CovFeFe?
Competing vaxxes, such as this one, are hindered by the mandates, which result in a lack of unvaxxed subjects for the clinical trials.
“The vaccine’s human trials took longer than expected, he said, because the lab needed to test the vaccine on subjects who had neither been vaccinated nor previously infected with COVID.”
ParticipantTDub: “The idea of shedding by the vaxxed… how would shedding work? Is it common for people to shed through respiration things that are in their bloodstream?”
I don’t know, maybe via the salivary glands?
“In vaccines, such as mRNA vaccines, the translated SP [Spike Protein] is released into interstitial fluid/blood, distributed to many organs and triggers an immune response… Herein, we show that SP [Spike Protein] had a body-wide biodistribution [in mice], slow regional elimination, except for the liver, which showed an accumulation, and differential organ uptake…. Also, SP [Spike Protein] was present in the salivary glands… There was significant SP [Spike Protein] signal in the salivary glands..”
Spike protein multiorgan tropism suppressed by antibodies targeting SARS-CoV-2
https://www.biorxiv.org/content/10.1101/2021.07.30.454520v1.fullParticipantA judge ruled that Covid vaxx mandates can’t be imposed by California school districts, it’s up to the state legislature.
ICAN-Funded Lawsuit Strikes Down COVID-19 Vaccine Mandate for San Diego Schools!
https://www.icandecide.org/ican_press/ican-funded-lawsuit-strikes-down-covid-19-vaccine-mandate-for-san-diego-schools/ParticipantWES: “Notice that preventative measures (vit D3, zinc, ivermectin) are not on the table in all of this!”
Yes, as explained by the study I posted above,
“Paradigm 1 implies that a public perception that therapeutics might reduce the severity of COVID-19 would be dangerous if it led to the premature lifting of NPIs [non-pharmaceutical interventions including “lockdowns”, “stay-at-home” orders, travel restrictions, mask-wearing, and regulated social distancing..]”
ParticipantLooking at two different “scientific” approaches to dealing with Covid-19, one is mostly model-driven, and the other is mostly empirical. “Remarkably, we find using each paradigm leads to diametrically opposite conclusions…”
Abstract
During the COVID-19 pandemic, many governments have adopted responses revolving around the open-ended use of non-pharmaceutical interventions (NPIs), including “lockdowns”, “stay-at-home” orders, travel restrictions, mask-wearing, and regulated social distancing. Initially these were introduced with the stated goals of “flattening the curve” of hospital demand and/or the eradication of the virus from the country (i.e., “zero covid” policies). Over time, these goals have shifted to maintaining sufficient NPIs in place until such time as population-wide vaccination programmes have achieved an appropriate level of herd immunity to allow lifting of these measures without excessive hospital demand. Supporters of this approach have claimed to be “following the science”, insisting that criticism of any aspects of these measures is non-scientific or even “scientific misinformation”. This idea that only one set of scientifically valid opinions on COVID-19 exists has encouraged the media, social media and even scientific journals to suppress and/or dismiss any differing scientific opinions as “erroneous”, “discredited” or “debunked”, resulting in discouragement of open-minded scientific inquiry or discussion. Accordingly, in the current article we identify two distinct scientific paradigms to analysing COVID-19 adopted within the medical and scientific community. Paradigm 1 is primarily model-driven, while Paradigm 2 is primarily empirically-driven. Using these two paradigms we have analysed the epidemiological data for 30 northern hemisphere countries (with a total population of 882 million). Remarkably, we find using each paradigm leads to diametrically opposite conclusions on many policy-relevant issues. We discuss how these conflicting results might be reconciled and provide recommendations for scientists and policymakers.
…
Paradigm 1, mostly model-driven, implies that non-pharmaceutical interventions (NPIs) are effective and essential until a population-wide vaccination programme has been completed. By corollary, Paradigm 1 implies that a public perception that therapeutics might reduce the severity of COVID-19 would be dangerous if it led to the premature lifting of NPIs.Paradigm 2, mostly empirically driven, is unable to find compelling evidence that the NPIs are particularly effective, but plenty of evidence that “the cure is worse than the disease”. Meanwhile, Paradigm 2 finds no need for a population-wide vaccination programme, although smaller-scale voluntary vaccination programmes may potentially be helpful in shielding the vulnerable and health-care workers. Paradigm 2 also implies that research into identifying effective therapeutics to reduce the severity of COVID-19 should be actively encouraged.
A TALE OF TWO SCIENTIFIC PARADIGMS: CONFLICTING SCIENTIFIC OPINIONS ON WHAT “FOLLOWING THE SCIENCE” MEANS FOR SARS-COV-2 AND THE COVID-19 PANDEMIC
AUTHORS Gerry A Quinn, Ronan Connolly, Coilín ÓhAiseadha, Paul Hynds
https://osf.io/s9z2p/ParticipantIn Ontario, fully-vaxxed case numbers have dramatically increased this past week:
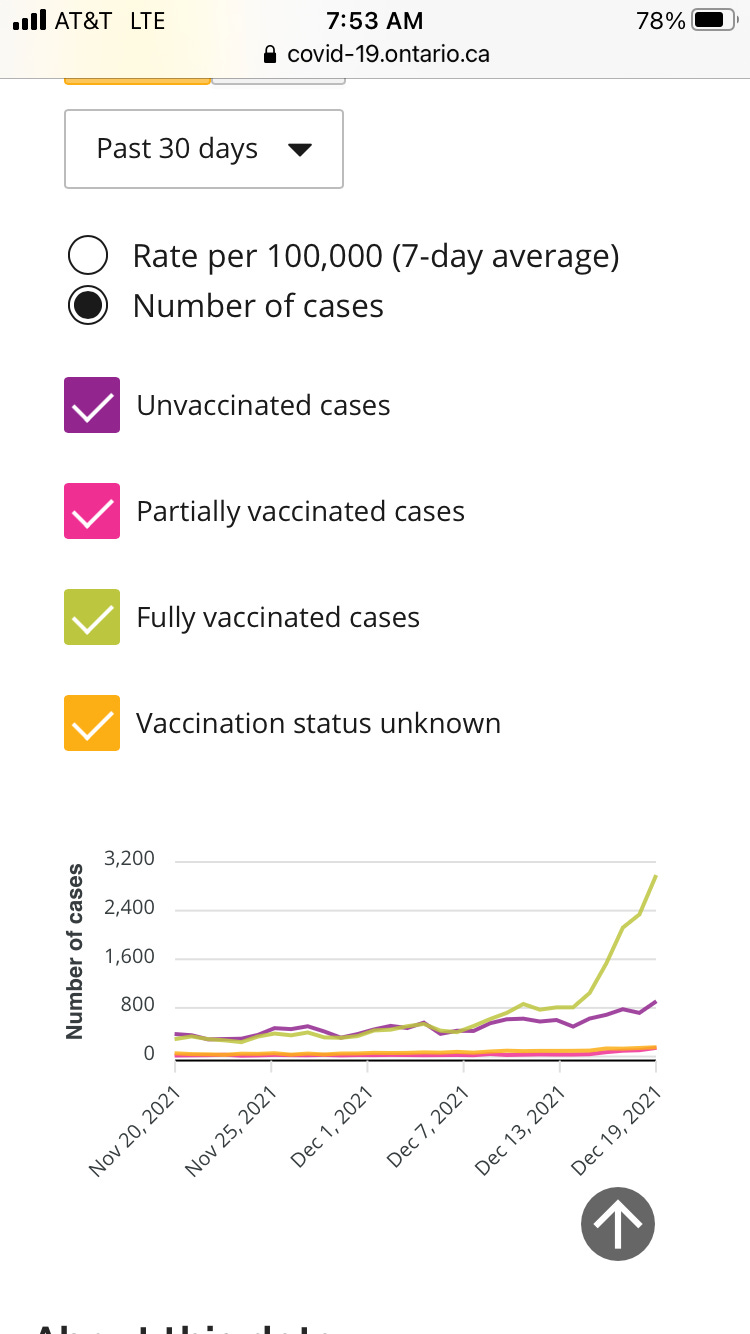
https://alexberenson.substack.com/p/stunning-data-about-vaccine-failure/commentsParticipantAn updated report from South Africa gives an earlier date for the first detection of Omicron:
October 24Variant of Concern Omicron
• South Africa:
• Earliest detection ca: 24 October, Eastern Cape
• Dominated November sequencing data at 81% of genomes (n=881/1082)
• Detected in all provinces
• Global:
• Detected in 88 countries worldwide
• Split into three lineages based on different mutational profiles: BA.1 (21K), BA.2 (21L), BA.3Network for Genomic Surveillance in South Africa (NGS-SA)
SARS-CoV-2 Sequencing Update 17 December 2021
https://www.nicd.ac.za/wp-content/uploads/2021/12/Update-of-SA-sequencing-data-from-GISAID-17-Dec-21_Final.pdfParticipantOmicron is such a problem that we barely notice when it’s here. A county in Florida (which includes Orlando) reported that nearly 100% of Covid strains in wastewater samples are omicron, while “those who are hospitalized are being primarily infected by the delta variant.”
A sampling this week showed that omicron represented almost 100% of the strains in the samples from the wastewater facilities, Orange County Utilities spokesperson Sarah Lux said in an email.
It’s a different story when it comes to people seeking treatment for COVID-19, officials said.
“Those who are hospitalized are being primarily infected by the delta variant”
Omicron is dominant in wastewater samples in Florida county
https://apnews.com/article/coronavirus-pandemic-health-travel-lifestyle-florida-e7907660a6d3ce352990ed151ba1a225ParticipantRegarding the hospitalizations graph, posted above:
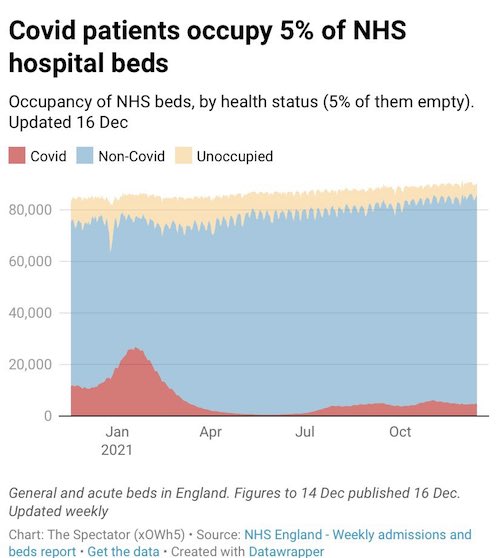
Q: Even if the Covid cases (in red) use only 5% of the hospital beds, aren’t most of the recent Covid hospitalizations unvaxxed?
A: No.The most recent official published data (covering the past few weeks) indicates that less than half of the NHS Covid hospitalizations are “not vaccinated.”
Table 9. COVID-19 cases presenting to emergency care (within 28 days of a positive specimen) resulting in an overnight inpatient admission by vaccination status between week 46 and week 49 2021
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1041593/Vaccine-surveillance-report-week-50.pdfParticipantredshift: “How do you get this figure? Based on worldometer I get 2.13% case closed fatality rate.”
The infection fatality rate (IFR) include the milder Covid infections which weren’t tested and not added to the official case numbers. The numbers in this table come from a worldwide study from 2020 published in the journal Nature. (I think the fatality rates have decreased since then.)
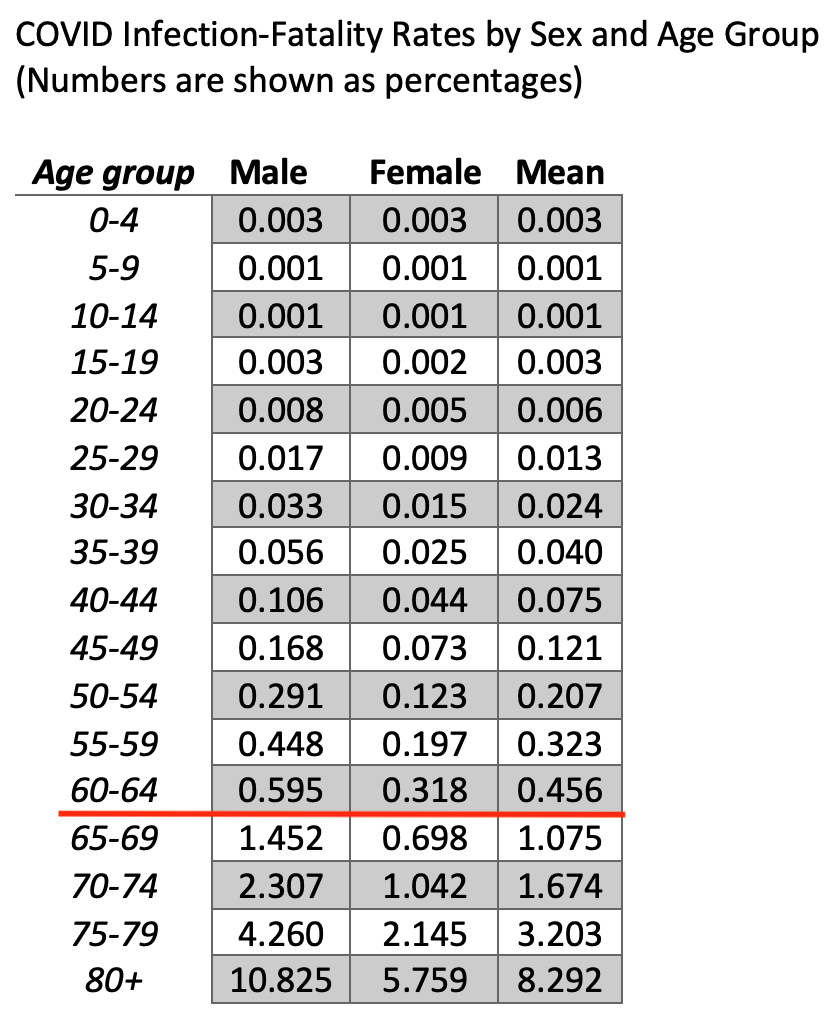
I don’t know where the .00189% number comes from, according to this table it would apply to someone in their teenage years. If it’s a typo and is meant to be 0.189% then according to the table it would apply to someone in the 50-54 age group.
Participant• BNT162b2 mRNA Vaccine Reprograms Adaptive And Innate Immune Responses (medRxiv)
From the full text of the study, the mRNA vaxx could interfere with the flu shots and cause as-yet unknown effects, “so it is crucial to perform additional studies“. Reminds me of FDA advisor Eric Rubin’s infamous words (about injecting the mRNA into young children), We’re Never Going To Learn About How Safe The Vaccine Is Until We Start Giving It..
The effect of the [Pfizer] BNT162b2 vaccination on innate immune responses may also indicate a potential to interfere with the responses to other vaccinations, as known for other vaccines to be as ‘vaccine interference’… Future studies are therefore needed to investigate this possibility, especially the potential interaction with the influenza vaccine: in the coming years (including the autumn of 2021) COVID-19 vaccination programs will probably overlap with the seasonal Influenza vaccination, so it is crucial to perform additional studies to elucidate the potential interactions and effects of the COVID-19 vaccines with the current vaccination schedules, especially for immunosuppressed and elderly individuals.
https://www.medrxiv.org/content/10.1101/2021.05.03.21256520v1.full-text
Participant• Pfizer Vaccine Reprograms Both Adaptive And Innate Immune Responses (Rose)
FWIW, I highly recommend that article by Dr Jessica Rose. Who is she?
Dr. Jessica Rose is a Canadian researcher with a Bachelor’s Degree in Applied Mathematics and a Master’s degree in Immunology from Memorial University of Newfoundland. She also holds a PhD in Computational Biology from Bar Ilan University and 2 Post Doctoral degrees: one in Molecular Biology from the Hebrew University of Jerusalem and one in Biochemistry from the Technion Institute of Technology.
That article gives some great explanations of how the immune system works and how it’s affected by the mRNA vaxxes.
Let’s assume the role of the coronavirus and see what our life would be like in the case of say, a child… And just so you know, there are many of me. So I find my way in a misty droplet into the sweet nasal cavity of this child where I encounter lots of mucousy membranes and sheets of epithelial cells. Lots of mucous. Mucosaliscious. I imagine it would be like running through a tunnel full of spider webs like Frodo Baggins did when he was trying to escape ‘she who needs to feed’ in order to get to the Mordor volcano to destroy the ring of power. So it’s kind of hard to get through. The nose. Sort of.
Ok, so most of me gets stuck in the booger path in the child’s nose. But nasal epithelial cells are chock full of ACE-2 receptors. I can bind them and thus can easily get inside the nice and warm cozy cells. There are also CD147 receptors here! So, a few of me manage to get ‘past’ this mucousy hurdle and bind to yummy epithelial cells via ACE-2 and CD147 receptors, which to me, are like red and yellow-colored lollipops of delight leading me into the place where I can call home and settle down and reproduce. But wait, before we get into that, since I am lurking around looking for receptors to bind, I am also encountering a lot of cells. These cells start telling me that they need to see my green pass if I want to keep lurking. No wait, no not my green pass, my PAMPs, so that they can find out how dangerous I am. I am new to this neck of the woods so they’re more than a little curious about my lurking. So they probe me with their PRR/TLR tools. Oh man! This is not pleasant at all! Being frisked by dendritic cells is like being manhandled by an octopus on a mission. So even though I have no idea, the by-product of their frisk is the inevitable launch of an army of things hell-bent on removing me from this kid. All of a sudden I’m surrounded by tenticular cells and they’re throwing TNF-alpha and IL-1 molotov cocktails at me! And it’s starting to get really hot in here and I’m like, man, this is not a hospitable environment. What did I do to deserve this? I’m just an innocent virus ultimately looking for a place to… breed.
Luckily, I have made a home in some cells. I am bound to others about to gain entry. But, the immune defenses don’t stop on the outside of cells; they continue on the inside. I thought I had found a nice warm and cuddly cell to settle down in and reproduce in. I have to think again! All of a sudden the PH is like, way too high! This feels awful! They’re trying to kill me, man! And eventually, they destroy me before I can get out. One of them sicked this crazy MAC on me and it poked holes in my home cell that I had managed to get into. They also used all sorts of internal and external armaments to make sure they cleared me out. And they did!
How do I know that? Because I am speaking from virus heaven.
So that’s the imaginary journey of the SARS-nCoV-2 virus and the potent response of a child’s innate immune system to my presence. Not enough cells get infected fast enough for an infection to ensue. The kid never gets to disease state and in most cases, symptoms are excessively mild or non-existent.
Alas, not enough of me were able to ‘infect’ enough cells to result in enough of me being produced to result in a ‘symptomatic infection’ party party. Innate immune system: 1. Coronavirus me: 0.
‘The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses’ It’s all in the title…
https://jessicar.substack.com/p/the-bnt162b2-mrna-vaccine-againstParticipantVeracious Poet: “Does anyone know how tweakers & opium addicts may be adversely effected by the mRNA cocktails? Wouldn’t they have an elevated risk?”
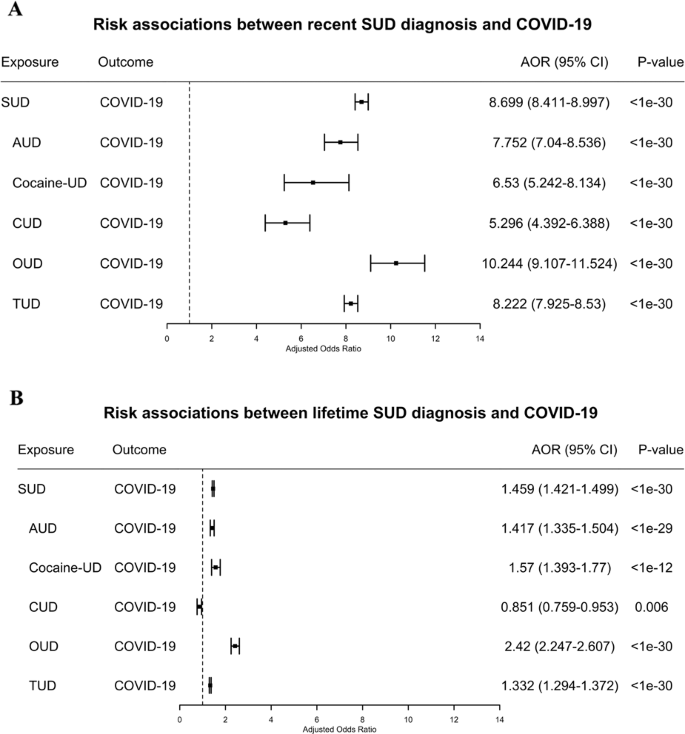
I don’t know about the effects of the mRNA injections on addicts, but a large study from 2020 found that people with an Opiod Use Disorder during the past year had more than 10 times the risk for a Covid infection. And Covid patients with Substance Use Disorders (SUD) had “significantly worse outcomes.”
Bucking the trend were people with a past history (not in the most recent year) of “Cannabis Use Disorder”, “Cannabis dependence (disorder)” or “Cannabis abuse (disorder)”; they had less chance of Covid infection (85% as likely), compared to the general population.
Patients with a recent diagnosis of [Substance Use Disorder] SUD (within past year) were at significantly increased risk for COVID-19 (adjusted odds ratio or AOR = 8.699…, an effect that was strongest for individuals with [Opioid Use Disorder] OUD (AOR = 10.244…), followed by individuals with tobacco use disorder (TUD) (AOR = 8.222…). Compared to patients without SUD, patients with SUD had significantly higher prevalence of chronic kidney, liver, lung diseases, cardiovascular diseases, type 2 diabetes, obesity and cancer… COVID-19 patients with SUD had significantly worse outcomes (death: 9.6%, hospitalization: 41.0%) than general COVID-19 patients (death: 6.6%, hospitalization: 30.1%)
COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States
https://www.nature.com/articles/s41380-020-00880-7Participant• Moderna CMO: Delta and Omicron Could Combine to Create ‘Monster’ Virus
Hyping up a hypothetical combo of variants, which is beyond our control, while shrugging off the very real occurrences of adverse reactions to the mRNA injections which are not beyond our control, since they are taken voluntarily (in most cases, unless it’s forced on you as a child).
Participant…and the number of deaths by suicide are much higher than the Covid deaths, for the 19-39 age group (BC Canada data).
ParticipantFor ages 0-59, the Covid deaths are dwarfed by the number of deaths due to “illicit drug toxicity.”
Top 15 causes of death by age group in BC Canada for March 2020 to October 2021
https://pbs.twimg.com/media/FGSi04iVQAEmXv2?format=png&name=smallParticipantAbout that list of airline pilot deaths, as Steve Kirsch puts it, “However, they only list the “new” deaths they heard about in each issue. So let’s not jump to conclusions just yet…We have a team of 40 people looking at all the back issues of the magazine and researching all the deaths. Stay tuned for what they find.”
https://stevekirsch.substack.com/p/are-100-dead-us-airline-pilots-trying
Participant• Why You Can’t Get COMIRNATY (Steve Kirsch)
Straight from CDC.GOV and current as of December 10:
COMIRNATY still cannot be ordered in the US.
Pfizer isn’t planning to make any COMIRNATY for US distribution over the next few months, while the unapproved EUA-authorized product is being made available by Pfizer.
It’s up to Pfizer to determine, at some time in the future, when the approved COMIRNATY will be made available in the US.
COMINARTY products are not orderable at this time. NDCs are listed per FDA Structured Product Label (SPL) document for the BLA licensed product. These codes are not included in CDC Vaccine Code Set files at this time. Pfizer has provided the following statement regarding the COMINARTY branded NDCs and labels:
“Pfizer received FDA BLA license on 8/23/2021 for its COVID-19 vaccine for use in individuals 16 and older (COMIRNATY). At that time, the FDA published a BLA package insert that included the approved new COVID-19 vaccine tradename COMIRNATY and listed 2 new NDCs (0069-1000-03, 0069-1000-02) and images of labels with the new tradename.
At present, Pfizer does not plan to produce any product with these new NDCs and labels over the next few months while EUA authorized product is still available and being made available for U.S. distribution. As such, the CDC, AMA, and drug compendia may not publish these new codes until Pfizer has determined when the product will be produced with the BLA labels.”https://www.cdc.gov/vaccines/programs/iis/COVID-19-related-codes.html
ParticipantCraig Murray is out of prison and back at his blog, with new details of the case against Julian Assange:
The effect of the judgement is that the case is now returned to Judge Baraitser with the instruction to reverse her decision and order Assange’s extradition. In doing so she passes the papers up to the Home Secretary, Priti Patel, with whom the final decision on all extraditions lies. Julian has until 23 December to submit an appeal against this High Court decision to the Supreme Court, something he is minded to do.
Now read this very carefully. The United States Government’s appeal to the High Court was only on those points on which Baraitser had ruled against extradition – Assange’s mental health and the effect upon it of extradition and US prisoner conditions. Assange’s appeal now to the Supreme Court will also be restricted to those subjects. The points on which Baraitser originally ruled in favour of the United States, including Assange’s First Amendment protections and the right of freedom of speech, the bar on political extradition and the inapplicability of espionage charges to journalism – will only be heard later, if he loses at the Supreme Court on what is still the US appeal.
If the Supreme Court decides for the US on the basis of diplomatic assurances, and the case returns to Baraitser to exercise the extradition warrant, at that time we finally have the cross appeal on all the issues this case is really about. If the High Court then accepts the cross-appeal as arguable (and Holroyde stated specifically that Assange’s wider points of appeal “would be heard at a later stage in proceedings”), then Patel’s trigger itching hand will be stayed while we restart the appeals process, quite possibly back to Holroyde and Burnett.
This benefits the Machiavellian state in two ways. For up to another year the legal argument will continue to be about Julian’s mental health, where the self-disparagement required by his defence suits the state political narrative. Nobody inside court is currently permitted to be talking about freedom of speech or the exposure of US war crimes, and that of course feeds in to the MSM reporting.
The state also is happy that this convoluted Supreme Court and then cross-appeal process will last for years not months, even before we look at the European Court of Human Rights, and all that time Julian Assange is stuck in high security in Belmarsh jail, treated as a terrorist, and his mental and physical health are visibly deteriorating in a way that is simply horrible. It is not hyperbole to state we may well be watching his slow murder by the state.
Your Man Back in the Public Gallery: Assange Extradition, US Appeal Result
https://www.craigmurray.org.uk/archives/2021/12/your-man-back-in-the-public-gallery-assange-extradition-us-appeal-result/ParticipantDr. D: “Tell me how you claim the delivery of $52T in resources? The whole planet isn’t worth that much.”
Reminds me of a laid-back comedian from Finland, named Ismo, who gives his analysis of the world debt situation:
Participantchooch: “…how the booster uptake in Japan is going. They started their rollout on Dec. 1st.”
This graph shows all shots, including boosters. Japan’s daily Covid shots have been declining, getting close to zero, and since December 1st, the downward trend has continued.
https://ourworldindata.org/grapher/daily-covid-vaccination-doses-per-capita?country=JPN~GBR~USA
ParticipantWill repeated Covid boosters lead to autoimmune problems? Some clues from a 2009 study:
“Systemic autoimmunity appears to be the inevitable consequence of over-stimulating the host’s immune ‘system’ by repeated immunization with antigen, to the levels that surpass system’s self-organized criticality.”
The present findings are consistent with the current consensus that CD4+ T cells normally die via activation-induced cell death (AICD) after repeated exposure to a single antigen, while naïve CD4+ T cells having a ‘cross-reactive’ TCR with lower affinity can be activated through repeated exposure to the same antigen and survive due to weak TCR signaling, ultimately acquiring autoreactivity [20]. We show here, however, that aiCD4+ T cells are induced not by cross-reaction, but by de novo TCR revision. The aiCD4+ T cells thus generated induce not only autoantibodies but also full-maturation of CD8+ T cells leading to autoimmune tissue injury akin to human SLE…
The question of how autoimmunity is triggered can therefore be deduced to the quantitative response of host against immunizing antigen, i.e., the ability of host to present and/or cross-present antigen. It then follows that the ability of certain antigens such as measles virus to cause autoimmunity may be due to their ability, in conjunction with its ability to present antigen, to overstimulate CD4+ and/or CD8+ T cells of certain hosts beyond integrity of their immune system…
Self-Organized Criticality Theory of Autoimmunity
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC2795160/ -
AuthorPosts
